SAGES
Reimagining surgical care for a healthier world
Construction of the gastric conduit.
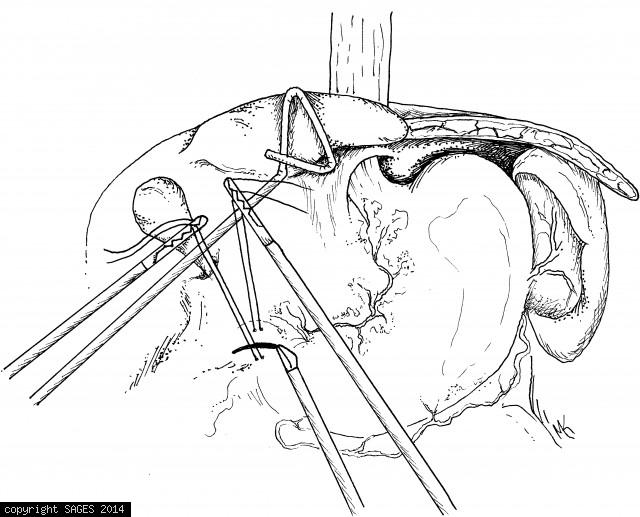
Pyloroplasty: closure of pylorus.
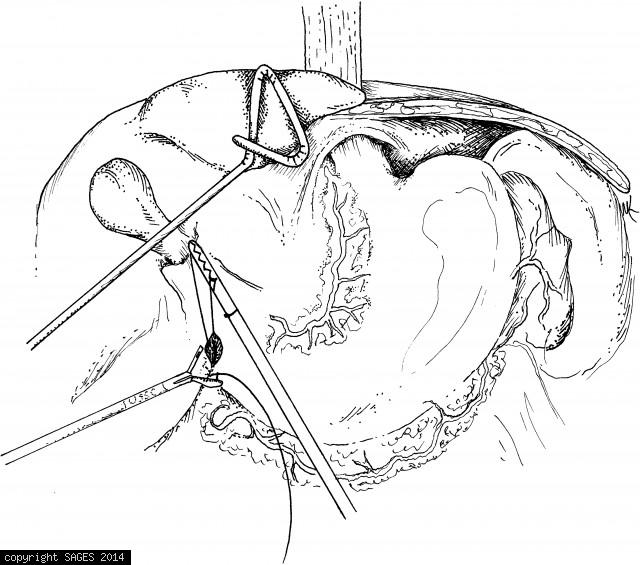
Pyloroplasty: opening of the pylorus
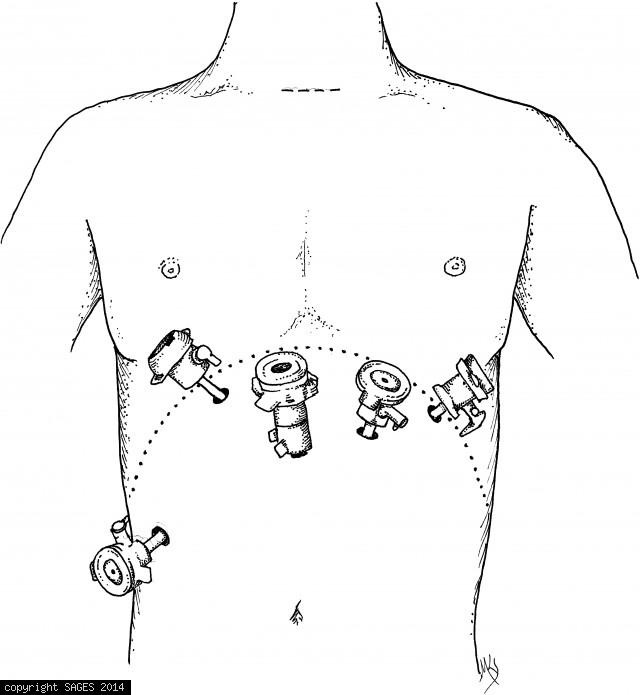
Port placement for gastric mobilization and tubularization.
Room setup for gastric mobilization and tubularization.