BACKGROUND: A leak at the gastrojejunal anastomosis (GJ) is a well recognized and occasionally fatal complication of obesity surgery. Closed suction drains have been routinely placed in the region of the GJ at the time of laparoscopic Roux-en-Y gastric bypass (LRYGBP) in order to aid in the recognition and treatment of such leaks. However, drains can increase pain, cost and operative time, and do not always fulfill their desired function.
METHODS: A retrospective review of 434 consecutive patients who had undergone LRYGBP from November 2000 through December 2006 by two fellowship trained laparoscopic surgeons at Penn State Milton S. Hershey Medical Center was performed. In all cases, a total linear stapled antecolic antegastric LRYGBP was performed and a 10 Fr Jackson Pratt drain was left in place alongside the GJ after omental wrap. Data were analyzed to determine the frequency of GJ leaks in this population, as well as to evaluate the efficacy of closed suction drains in the diagnosis and management of such leaks. Drains were removed in stable patients after 24 hrs of oral intake. A contrast study was obtained on selected patients only if clinically indicated to evaluate for leak.
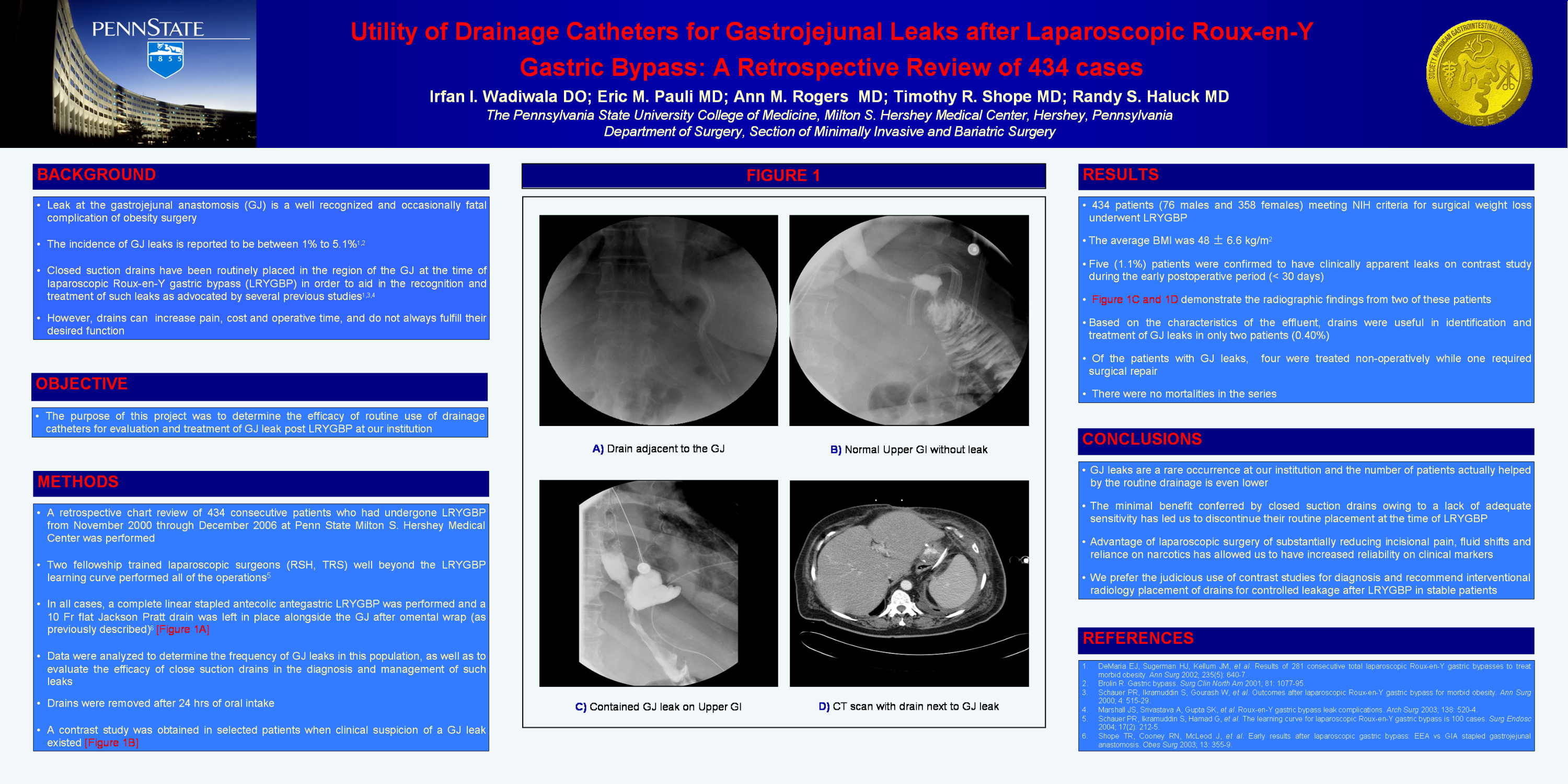
RESULTS: 434 patients (76 males and 358 females) meeting NIH criteria for surgical weight loss underwent LRYGBP. The average BMI was 48 ± 6.6. Five (1.1%) patients were confirmed to have clinically apparent leaks on contrast study during the early postoperative period (< 30 days). Based on the characteristics of the effluent, drains were useful in identification and treatment of only two of these patients (0.40%). Four patients were treated nonoperatively while one required surgical repair. There was no mortality in the series.
CONCLUSIONS: GJ leaks are a rare occurrence at our institution. The minimal benefit conferred by closed suction drains owing to a lack of adequate sensitivity has led us to discontinue their routine placement at the time of LRYGBP. We prefer the judicious use of contrast studies for the diagnosis of leaks and recommend percutaneous placement of drains for controlled GJ leakage after LRYGBP in stable patients.
Session: Poster
Program Number: P025

{kind=link}