Piotr Gorecki, MD FACS, Krystyna Kabata, PA, Srikanth Eathiraju, MD, Suraj Parekh, MD, Anthony Tortolani, MD. NEW YORK METHODIST HOSPITAL
Introduction: Creation of gastrojejunostomy during laparoscopic gastric bypass remains technically challenging part of the procedure. The techniques utilized include: circular stapled anastomosis (CSA), linear stapled anastomosis (LSA), and hand sewn anastomosis (HSA). No consensus on optimal technique exists and individual surgeon’s training and personal preferences are main determinants behind the choice of method.
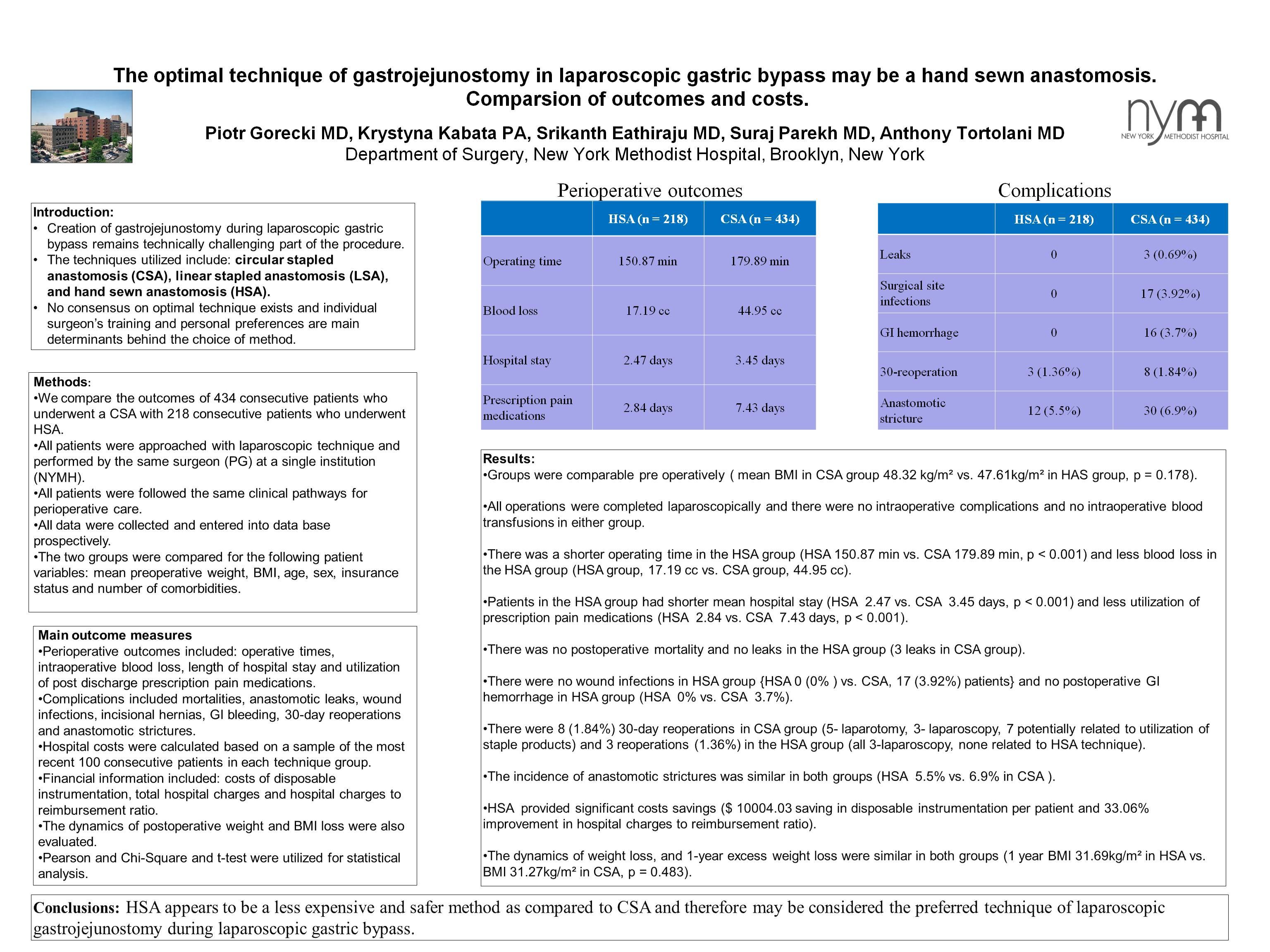
Methods: We compare the outcomes of 434 consecutive patients who underwent a CSA with 218 consecutive patients who underwent HSA. All patients were approached with laparoscopic technique and were performed by the same surgeon (PG) at a single institution (NYMH). All patients followed the same clinical pathways for perioperative care. All data were collected and entered into the data base prospectively. The two groups were compared for the following patient variables: mean preoperative weight, BMI, age, sex, insurance status and number of comorbidities.
Main outcome measures: Perioperative outcomes included: operative times, intra-operative blood loss, length of hospital stay and utilization of post discharge prescription pain medications. Complications included mortalities, anastomotic leaks, wound infections, incisional hernias, GI bleeding, 30-day reoperations and anastomotic strictures. Hospital costs were calculated based on a sample of the most recent 100 consecutive patients in each technique group. Financial information included: costs of disposable instrumentation, total hospital charges and hospital charges to reimbursement ratio. The dynamics of postoperative weight and BMI loss were also evaluated. Pearson Chi-Square and t-test were utilized for statistical analysis.
Results: Groups were comparable preoperatively (mean BMI in CSA group 48.34 vs. 47.61 in HSA group, p=0.178). All operations were completed laparoscopicaly and there were no major intraoperative complications and no intraoperative blood transfusions in either group. There was a shorter operating time in the HSA group (HSA group, 150.87 min vs. CSA group, 179.89 min, p<0.001) and less blood loss in the HSA group (17.19 cc vs. 44.95 cc.). Patients in the HSA group had shorter mean hospital stay (2.47 vs.3.45 days, p<0.001) and less utilization of prescription pain medications (2.84 vs. 7.43 days, p<0.001). There was no postoperative mortality and no leaks in the HSA group (3 leaks in CSA group). There were no wound infections in HSA group (HSA 0% vs. CSA, 17 patients, 3.92%), and no postoperative GI hemorrhage in HSA group (0% vs.3.7%). There were 8 (1.84%) 30-day reoperations in CSA group (5-laprotomy, 3- laparoscopy, 7 potentially related to utilization of staple products) and 3 reoperations (1.36%) in the HSA group (all 3 – laparoscopy, none related to HSA technique). The incidence of anastomotic strictures was similar in both groups (HSA 5.5% vs. 6.9% in CSA group). HSA provided significant costs saving ($1004.03 saving in disposable instrumentation per patient) and 33.06% improvement in hospital charges to reimbursement ratio. The dynamics of weight loss, and 1-year excess weight loss were similar in both groups (1 year BMI 31.27 in CSA vs. BMI 31.69 in HSA, p=0.483)
Conclusions: HSA appears to be a less expensive and safer method as compared to CSA and therefore may be the preferred technique of laparoscopic gastrojejunostomy during laparoscopic gastric bypass.
Session Number: Poster – Poster Presentations
Program Number: P496
View Poster