Jose Luis Ibarrola-Calleja, MD, Mauricio Rodriguez-Gonzalez, MD, Miguel Eljure-Eljure, MD, Jaime Ordones, MD. hospital Angeles del pedregal in Mexico City
Since Boerhaave’s description of an esophageal perforationin 1724, these pathologic conditions are associated with a high mortality rate and their prognosis depends on the site of perforation and the time elapsed before reatment is instituted. If immediate treatment is performed, mortality runs at about 5%, raising to 14% if treated within 24 hours and to 44% if treated afterwards.
Upper G-I endoscopy is the most frequent cause of esophageal perforation (40 to 59% of all perforations), although it only occurs in 0.33% of all endoscopies, the most frequent site being the cervical esophagus.
X Ray studies are an important tool in the diagnosis: the presence of air within the neck’s soft tissues or pneumomediastinum (depending on the site of perforation) can be pathognomonic. Upper G – I endoscopy under anesthesia can show the type, site and extent of the perforation, and may suggest the adequate treatment. Ideal therapy is still debated, and the current conduct is to adapt the treatment to the patient’s conditions.
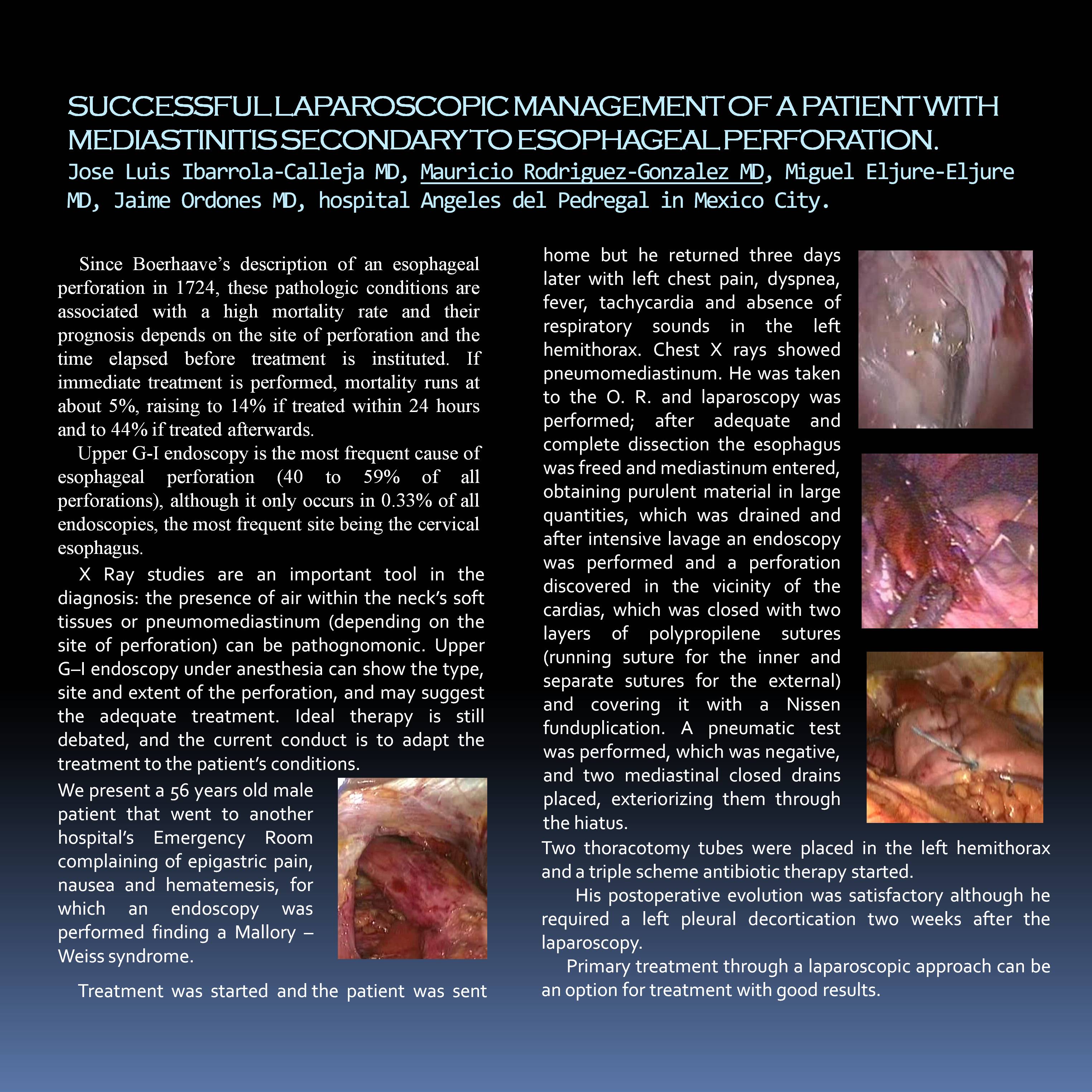
We present a 56 years old male patient that went to another hospital’s Emergency Room complaining of epigastric pain, nausea and hematemesis, for which an endoscopy was performed finding a Mallory – Weiss syndrome. Treatment was started and the patient was sent home but he returned three days later with left chest pain, dyspnea, fever, tachycardia and absence of respiratory sounds in the left hemithorax. Chest X rays showed pneumomediastinum. He was taken to the O. R. and laparoscopy was performed; after adequate and complete dissection the esophagus was freed and mediastinum entered, obtaining purulent material in large quantities, which was drained and after intensive lavage an endoscopy was performed and a perforation discovered in the vicinity of the cardias, which was closed with two layers of polypropilene sutures (running suture for the nner and separate sutures for the external) and covering it with a Nissen funduplication. A pneumatic test was performed, which was negative, and two mediastinal closed drains placed, exteriorizing them through the hiatus. Two thoracotomy tubes were placed in the left hemithorax and a triple scheme antibiotic therapy started.
His postoperative evolution was satisfactory although he required a left pleural decortication two weeks after the laparoscopy.
Primary treatment through a laparoscopic approach can be an option for treatment with good results.
Session: Poster
Program Number: P450
View Poster
{kind=link}