Aileen Murphy, MA DO, Satbir Dhillon, BS, Maureen Martin, MD FACS FRCSC. Department of Surgery, Kern Medical Center, Bakersfield, Ca
INTRODUCTION: Our center has adopted a policy of selective intraoperative cholangiography (SIOC) during laparoscopic cholecystectomy (LC). This study aimed to evaluate the incidence and management of choledocholithiasis, extrahepatic bile duct injuries, and other findings potentially affected by intraoperative cholangiogram (IOC).
METHODS AND PROCEDURES: Medical records were reviewed of patients undergoing cholecystectomy at our institution from July 2005 to July 2011. Dissection with the goal to achieve the critical view of safety was the standard operative technique for our patients.
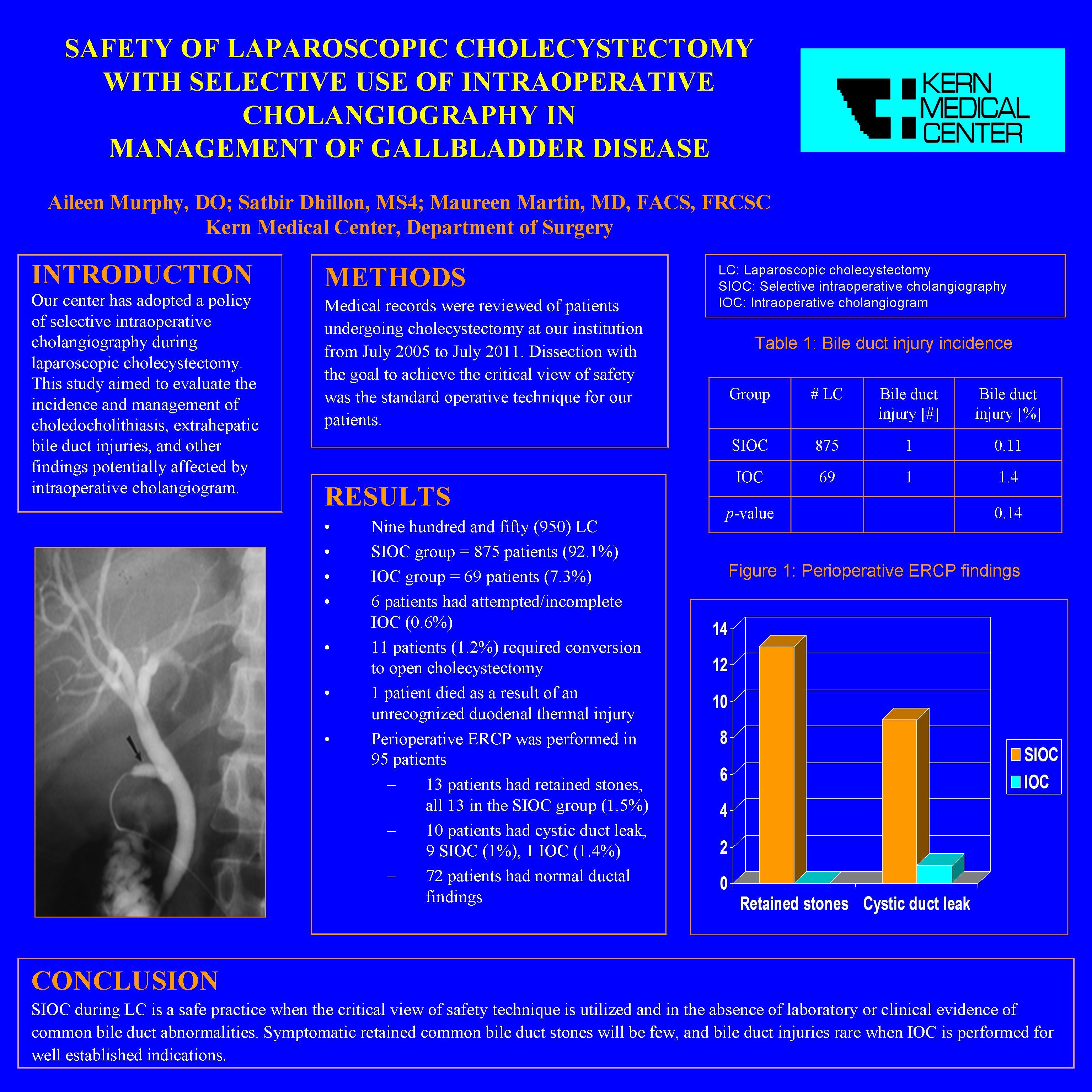
RESULTS: Nine hundred and fifty (950) patients underwent LC. Eleven (11) patients (1.2%) required conversion to open cholecystectomy. One (1) patient died as a result of an unrecognized duodenal thermal injury. Eight hundred and seventy five (875) patients received SIOC (92.1%), while sixty-nine (69) patients received IOC (7.3%) and six (6) patients had attempted IOC (0.6%). The rate of major bile duct injury was 1/875 (0.11%) in the SIOC group, and 1/69 (1.4%) in the IOC group, p=0.14. Perioperative ERCP was performed in 95 patients. Findings included 13 patients with retained stones, all 13 in the SIOC group (1.5%); 10 patients with cystic duct leak, 9 SIOC (1%), 1 IOC (1.4%); and 72 patients with normal ductal findings. Retained stones passed incidentally or were treated with endoscopic sphincterotomy when indicated.
CONCLUSIONS: SIOC during LC is a safe practice when the critical view of safety technique is utilized and in the absence of laboratory or clinical evidence of common bile duct abnormalities. Symptomatic retained common bile duct stones will be few, and bile duct injuries rare when IOC is performed for well established indications.
Session Number: Poster – Poster Presentations
Program Number: P359
View Poster