Tammy T Chang, MD PhD, Francesco Palazzo, MD, Quan-Yang Duh, MD. University of California, San Francisco, San Francisco, California, USA
INTRODUCTION: Laparoscopic inguinal hernia repair has certain advantages over open repair, including less post-operative pain and earlier return to normal activity. However, a prolonged surgeon learning curve has limited its more generalized application. Robotic-assisted surgery provides surgeons with improved three-dimensional visualization and enhanced dexterity with articulating instrumentation. Robot assistance may improve outcomes of minimally invasive inguinal hernia repairs. We present a series of robotic inguinal hernia repairs performed by one surgeon at a single institution to demonstrate the feasibility of the robotic approach. These cases were retrospectively matched to laparoscopic inguinal hernia repairs performed by the same surgeon during the same period. We compared operative time, cost, and early outcomes of the robotic versus laparoscopic procedure to determine whether robotics may have a role in the future of minimally invasive inguinal hernia repair.
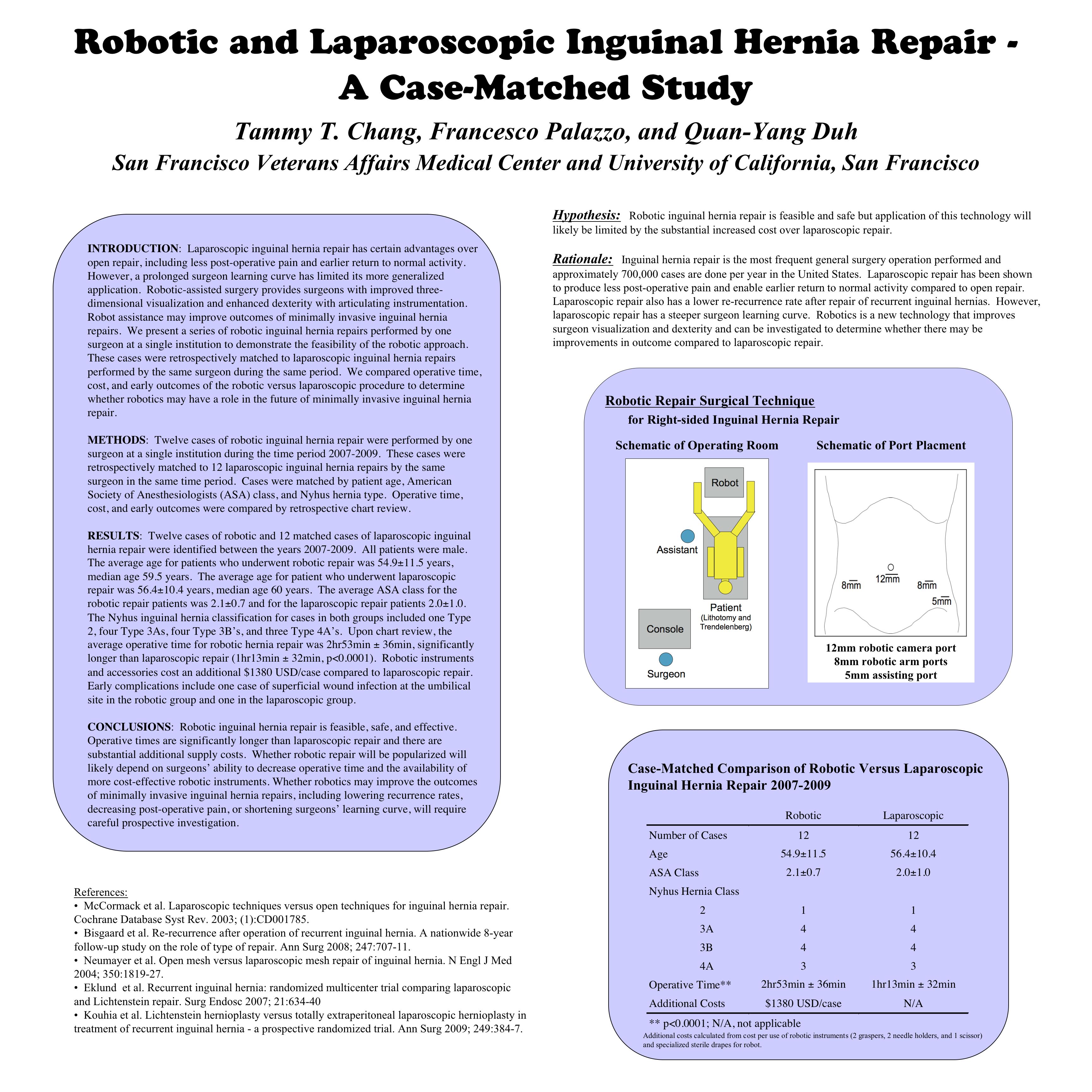
METHODS: Twelve cases of robotic inguinal hernia repair were performed by one surgeon at a single institution during the time period 2007-2009. These cases were retrospectively matched to 12 laparoscopic inguinal hernia repairs by the same surgeon in the same time period. Cases were matched by patient age, American Society of Anesthesiologists (ASA) class, and Nyhus hernia type. Operative time, cost, and early outcomes were compared by retrospective chart review.
RESULTS: Twelve cases of robotic and 12 matched cases of laparoscopic inguinal hernia repair were identified between the years 2007-2009. All patients were male. The average age for patients who underwent robotic repair was 54.9±11.5 years, median age 59.5 years. The average age for patient who underwent laparoscopic repair was 56.4±10.4 years, median age 60 years. The average ASA class for the robotic repair patients was 2.1±0.7 and for the laparoscopic repair patients 2.0±1.0. The Nyhus inguinal hernia classification for cases in both groups included one Type 2, four Type 3As, four Type 3B’s, and three Type 4A’s. Upon chart review, the average operative time for robotic hernia repair was 2hr53min ± 36min, significantly longer than laparoscopic repair (1hr13min ± 32min, p<0.0001). Robotic instruments and accessories cost an additional $1380 USD/case compared to laparoscopic repair. Early complications include one case of superficial wound infection at the umbilical site in the robotic group and one in the laparoscopic group.
CONCLUSIONS: Robotic inguinal hernia repair is feasible, safe, and effective. Operative times are significantly longer than laparoscopic repair and there are substantial additional supply costs. Whether robotic repair will be popularized will likely depend on surgeons’ ability to decrease operative time and the availability of more cost-effective robotic instruments. Whether robotics may improve the outcomes of minimally invasive inguinal hernia repairs, including lowering recurrence rates, decreasing post-operative pain, or shortening surgeons’ learning curve, will require careful prospective investigation.
Session: Poster
Program Number: P497
View Poster
{kind=link}