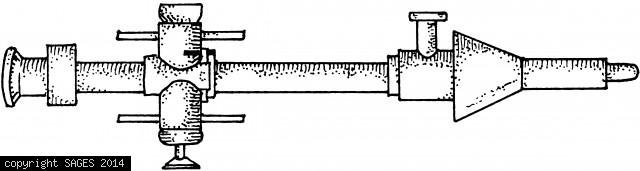
Tubing Placement

Diagram demonstrating the placement of flexible tubing or wire in combination with low-pressure pneumoperitoneum: (A) Banting et al. (1993), (B) Inoue et al. (1993), (C) Go et al. (1995). These techniques can be adapted using readily available materials a
Bleeding From Trocar Site
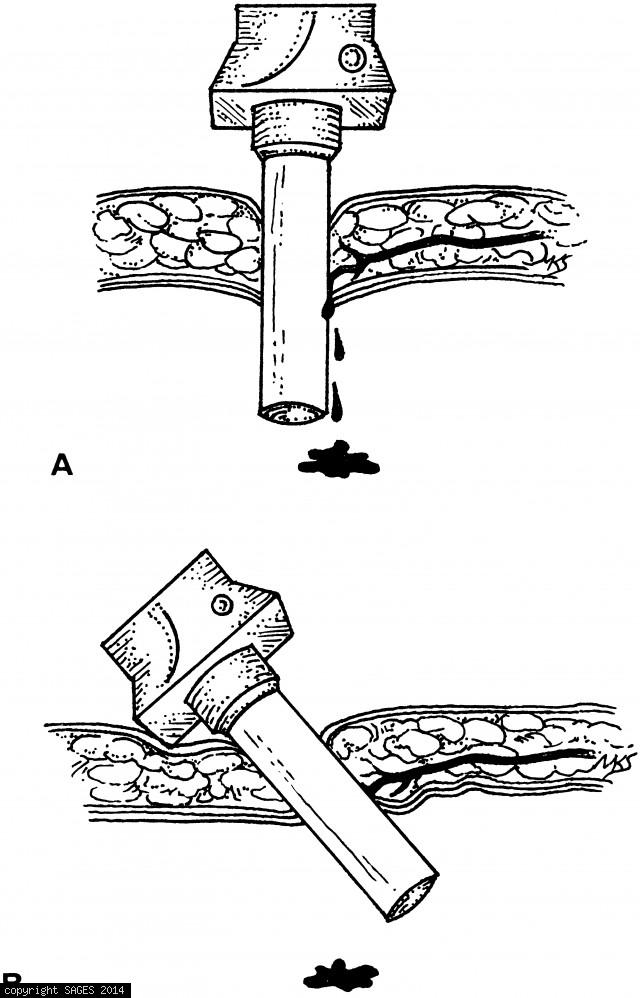
A. Bleeding from a trocar site. B. Cantilevering the sheath into each quadrant to find a position that causes the bleeding to stop. When the proper quadrant is found, pressure from the portion of the sheath within the abdomen tamponades the bleeding ve
Bleeding From Abdominal Wall
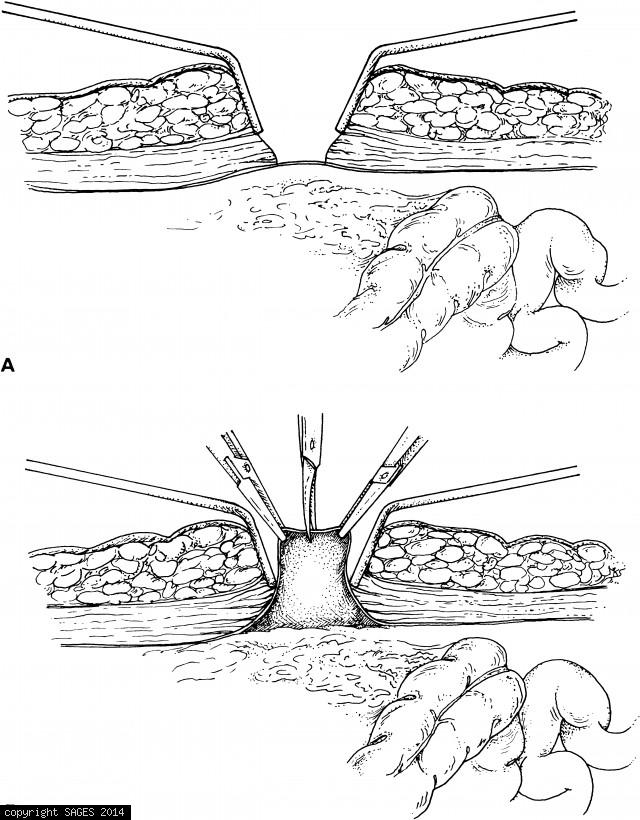
A. Retractors expose peritoneum. B. Peritoneum is elevated and sharply incised. Two fascial sutures are secured to the struts on the sheath of the open cannula. The cone-shaped sleeve is then pushed firmly into the incision and the setscrew is tightene
Trocar Sites
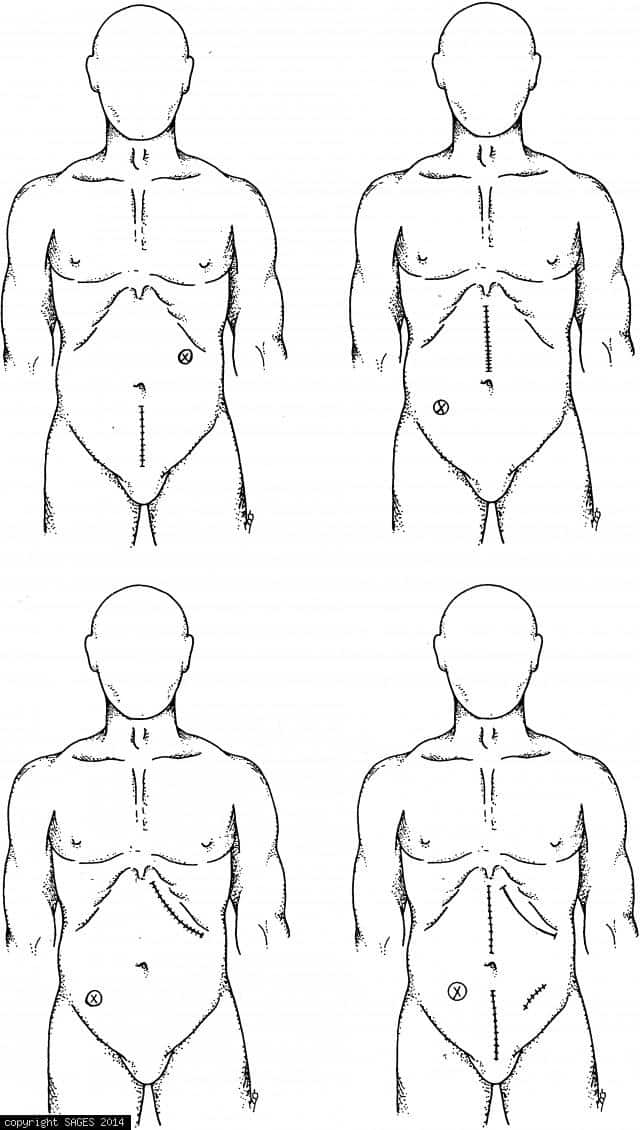
Optional trocar sites in previously operated abdomen. Consider the open-cannula technique.