
Introduction
Pneumothorax, the collection of gas within the pleural cavity, is caused either by trauma, infectious processes such as tuberculosis, or occurs spontaneously. Spontaneous pneumothorax occurs either on the basis of other underlying pathology, such as cystic fibrosis, emphysema, and connective tissue disease, or is considered primary if none of these predispositions are present. In primary spontaneous pneumothorax (PSP), macroscopically visible areas of weakness on the visceral pleura (so called blebs or bullae) are present in most patients, and often are bilateral [1].
PSP is up to 10 times more common in males than in females, with an annual incidence of about 20/100000 patients per year [2]. Risk factors are tall stature and low body mass index. Smoking is also am extrinsic risk factor.
Pathophysiology
Although PSP is defined as occurring without an identifiable etiology, it is still associated with certain structural changes of the lung and pleura. Typically, blebs and bullae are present, mostly in the apical areas of the lungs. In some cases, an unspecific chronic inflammatory process of the distal airways can be identified by histology [1,3].
Clinical Presentation and Evaluation
The typical patient is a tall, thin, male adolescent, complaining of sudden onset of sharp chest pain, sometimes associated with strenuous activity. The patient may exhibit tachypnea, but usually there is no clinically detectable cyanosis. A careful history about overt or possibly occult previous pneumothoraces should be taken, along with a family history of connective tissue disorders. If the patient exhibits clinical criteria for Marfan’s Syndrome, a cardiology consult and echocardiography may is indicated. In select cases, infectious and chronic diseases such as tuberculosis and cystic fibrosis should be considered and ruled out. Vital signs are assessed and supplemental oxygen should be promptly given for any signs of dyspnea, tachypnea, or low oxygen saturation.
PA and lateral chest radiographs are be obtained to assess for pneumothrorax. The severity of the pneumothorax, along with the patient’s symptoms, will determine the most appropriate treatment.
The number of anomalies detected on plain film radiographs (pleural thickening: blebs/bullae; pleural irregularities and pleural adhesions) correlates with the overall risk of recurrence [4].
Most practitioners reserve a computed tomography (CT) of the chest for patients presenting with recurrent pneumothorax.
Treatment
There is no universal consensus regarding treament of PSP. The overall recurrence risk for PSP is 30, 62, and 82% after the first, second, and third episodes, respectively [5]. Therefore, nonoperative management with either observation for small pneumothoraces, or catheter/chest tube drainage in symptomatic patients seems rational for the initial presentation. Operative intervention is warranted for patients return with more than one episode of pneumothorax, or individuals who plan to engage in high-risk activities (such as for example, flying or diving). Furthermore, bullae or blebs on diagnostic imaging are a compelling reason for resection and pleurodesis, since the recurrence rate is higher in those patients. A consensus statement on the treatment of specific clinical scenarios of primary spontaneous pneumothorax has been published and can serve as a guide [6].
Operative management consists of resection of any idetified blebs or bullae, along with pleurodesis or pleurectomy of the apical pleural cavity.
Bleb resection and pleurodesis via thoracoscopy or mini-thoracotomy has been shown to be equally effective in terms of recurrence rate, complication rate, and postoperative length of stay, although patient satisfaction after thoracoscopy was found to be higher [7].
Interestingly, blebs or bullae are found in only 71% of cases at the time of surgery, and an actual site of air leakage is only identified in 26% [3]. There is controversy if apical lung resection should be performed “blindly” if no visceral pleural anomalies are identified.
There also has been controversy on whether asymptomatic contralateral blebs found on CT should prompt the surgeon to perform bilateral resection and pleurodesis. However, in one study, the risk of recurrent pneumothorax decreased from 17% to 0% when the procedure was performed on both sides simultaneously during a follow-up time of 18 months [8]. Furthermore, in a pediatric study, all children with CT-proven blebs that did not have surgery on that side eventually presented with recurrence [9].
Although the resected tissue may show a variety of macroscopic and microscopic changes, the histolopathologic results did not alter subsequent clinical therapy in a study on 64 cases [10]. Therefore, the utility of sending the resected lung specimens for histologic analysis in cases with typical PSP is at least debatable.
Thoracoscopic Technique
The patient is placed in the contralateral decubitus position to the symptomatic side. Usually, a 3-trocar technique is performed. In most cases, 5 mm instruments and optics are used, particularly because they provide more purchase on the tissue than 3 mm instruments. The first trocar is placed in the 5th or 6th intercostal space at the mid-axillary line. The lung surface is inspected, and the other trocars are placed depending on the location of any obvious blebs. Because these are mostly found apically, placing them low in the chest usually allows for adequate working space and also facilitates pleurodesis of the upper portion of the hemithorax. If the surgeon plans to perform the blebectomy/lung resection with an endoscopic stapler, a trocar of adequate diameter must be placed strategically, particularly taking into account the distance of the angulation going from the jaws of the stapler if angulation is desired or necessary to reach the tissue. The thoracoscope should have an optical angle of 30° or 45° to allow for adequate inspection of all structures.
Selective lung intubation is not a requirement, but has been found to possibly decrease operating time and intraoperative complications rates in one study [11]. In most cases, insufflating the pleural space with carbon dioxide at a pressure around or slightly above PEEP can optimize the working space.
First, all lobes of the lung and its pleural surfaces are evaluated for blebs and bullae, as well as any other anomalies (figure 1). Most surgeons prefer to use the endoscopic stapler for resection of the lesions (figure 2), although endoscopic loop ties [12], and endoscopic suturing [13] have also been proposed. Once identifiable blebs and bullae have been resected, pleurodesis or pleurectomy is performed. For pleurodesis, a gauze sponge or a sterile electrocautery scatch pad can be used, abrading particularly the upper part of the pleural cavity. Some surgeons complement mechanical pleurodesis with a sclerosing agent such as minocycline, tetracycline, or talc. Alternatively, the parietal pleura can be stripped by incising it longitudinally using a hook cautery, then grasping the loose end with a grasper and “rolling” the pleura up around the instrument (figure 3). Pleurectomy and pleurodesis has been shown to be equally effective [14]. A chest tube is placed through one of the port sites and kept on suction for 24-48 hours to make sure that the lung is fully expanded and that the visceral surface adheres to the chest wall.

Figure 1: A bleb (long arrow) is visible on the left lower lobe in an adolescent with recurrent pneumothorax. A fibrinous strand (short arrow) is also noted leading towards the apex of the upper lobe where an area of scarred pleura was found as the sequellae of a previously ruptured bleb.

Figure 2: The lower lobe bleb is resected using the endosurgical stapler.
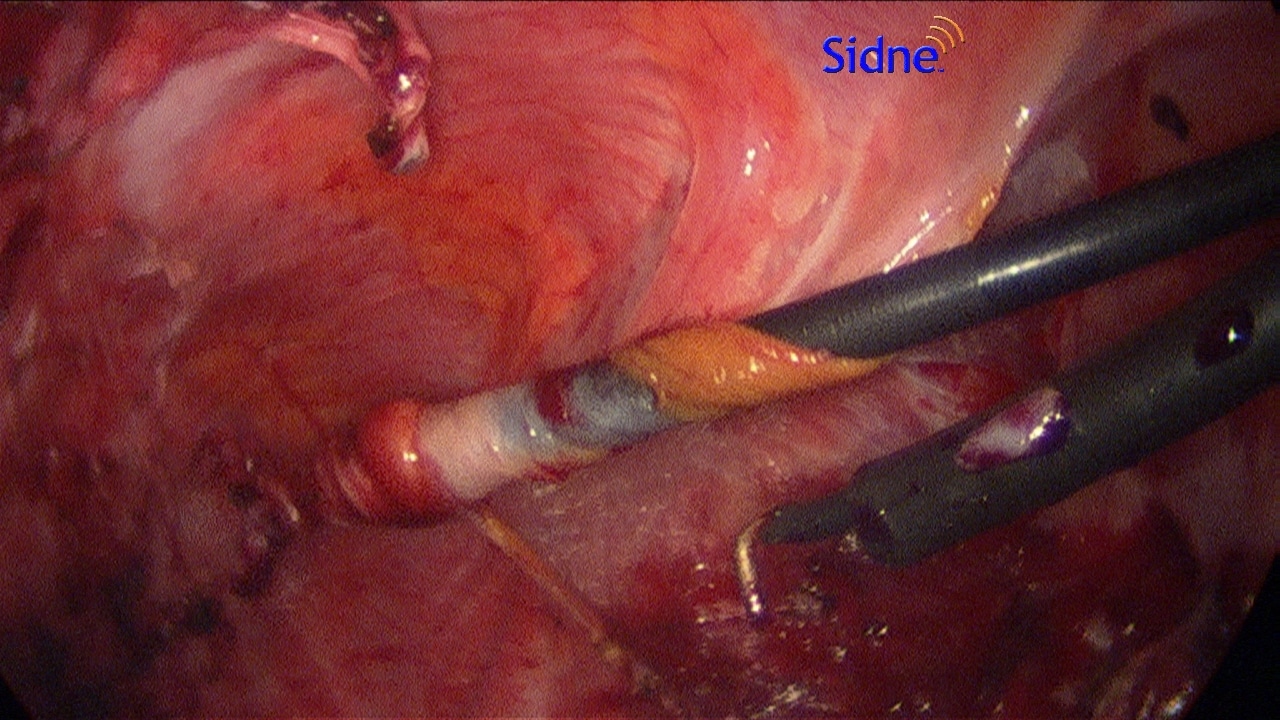
Figure 3: In this case, pleurectomy was performed by incising the pleura longitudinally with electrocautery, grasping the free edge and “rolling” it up on the grasper.
Postoperative Care and Complications
The recurrence rate is significantly higher in patients who undergo blebectomy alone compared to those who have a concomitant blebectomy and pleurodesis [15]. Overall, the postoperative recurrence rate is reported around 5% [3,16]. Other long-term complications are rare. Although there is a paucity of data on when commercial air travel is safe after surgical treatment of spontaneous pneumothorax, most authorities suggest waiting at least 2 weeks after radiographic resolution [17].
Summary
The treatment of recurrent spontaneous pneumothorax consists of surgical resection of blebs and bullae with concomitant pleurodesis or pleurectomy. While the thoracoscopic approach is at least as safe and effective as the open approach, it is associated with higher postoperative overall patient satisfaction.
References
1. Grundy S, Bentley A, Tschopp J. Primary spontaneous pneumothorax: A diffuse disease of the pleura. Respirateion 2012;83:185-9
2. MacDuff A, Arnold A, Harvey J: Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010;65:ii18–ii31
3. Ayed AK1, Chandrasekaran C, Sukumar M. Video-assisted thoracoscopic surgery for primary spontaneous pneumothorax: clinicopathological correlation. Eur J Cardiothorac Surg. 2006;29:221-5
4. Ganesalingam R1, O’Neil RA, Shadbolt B, Tharion J. Radiological predictors of recurrent primary spontaneous pneumothorax following non-surgical management. Heart Lung Circ 2010;19:606-10
5. Gobbel W. Spontaneous pneumothoorax. J Thorac Cardiovasc Surg 1963;46:331-45
6. Baumann MH1, Strange C, Heffner JE et al. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest 2001;119:590-602
7. Foroulis CN1, Anastasiadis K, Charokopos N et al. A modified two-port thoracoscopic technique versus axillary minithoracotomy for the treatment of recurrent spontaneous pneumothorax: a prospective randomized study. Surg Endosc 2012;26:607-14
8. Chou SH1, Li HP, Lee JY, Chang SJ et al. Is prophylactic treatment of contralateral blebs in patients with primary spontaneous pneumothorax indicated? J Thorac Cardiovasc Surg 2010;139:1241-5
9. Nathan N1, Guilbert J, Larroquet M et al. Efficacy of blebs detection for preventive surgery in children’s idiopathic spontaneous pneumothorax. World J Surg 2010;34:185-9
10. Khan OA1, Tsang GM, Barlow CW, Amer KM. Routine histological analysis of resected lung tissue in primary spontaneous pneumothorax — is it justified? Heart Lung Circ 2006;15:137-8
11. Cheng YL, Huang TW, Lee SC, et al. Video-assisted thoracoscopic surgery using single-lumen endotracheal tube anaesthesia in primary spontaneous pneumothorax. Respirology 2010;15:855-9
12. Liu YH, Chao YK, Wu YC et al. Bullae ablation in primary spontaneous pneumothorax. World J Surg 2009;33:938-42
13. Cheng YJ, Kao EL. Prospective comparison between endosuturing and endostapling in treating primary spontaneous pneumothorax. J Laparoendosc Adv Surg Tech A. 2004;14:274-7
14. Chen J, Hsu H, Huang P et al. Thoracoscopic Pleurodesis for Primary Spontaneous Pneumothorax With High Recurrence Risk: A Prospective Randomized Trial. Ann Surg 2012;255:440–5
15. Loubani M, Lynch V. Video assisted thoracoscopic bullectomy and acromycin pleurodesis: an effective treatment for spontaneous pneumothorax. Respir Med 2000;94: 888–90
16. Sakurai H. Videothoracoscopic surgical approach for spontaneous pneumothorax: review of the pertinent literature. World J Emerg Surg. 2008;3:23
17. Cheatham ML1, Safcsak K. Air travel following traumatic pneumothorax: when is it safe? Am Surg 1999;65:1160-4
Author
Oliver J. Muensterer, MD, PHD
Division of Pediatric Surgery
New York Medical College,
Valhalla, NY 10595
[email protected]