Toshiaki Shichinohe, MD PhD, Kentaro Kato, MD PhD, Akihiro Matsunaga, MD PhD, Satoshi Hayama, MD PhD, Takahiro Tsuchikawa, MD PhD, Joe Matsumoto, MD PhD, Takehiro Noji, MD PhD, Norihiro Takemoto, MD PhD, Yoshinori Suzuki, MD PhD, Hiroyuki Kaneko, MD PhD, Eiichi Tanaka, MD PhD, Satoshi Hirano, MD PhD. Gastrointestinal Surgery II, Hokkaido University Graduate School of Medicine, Sapporo, Japan.
Introduction
Video assisted thoracoscopic surgery (VATS) for thoracic esophageal cancer is an advanced surgical technique.
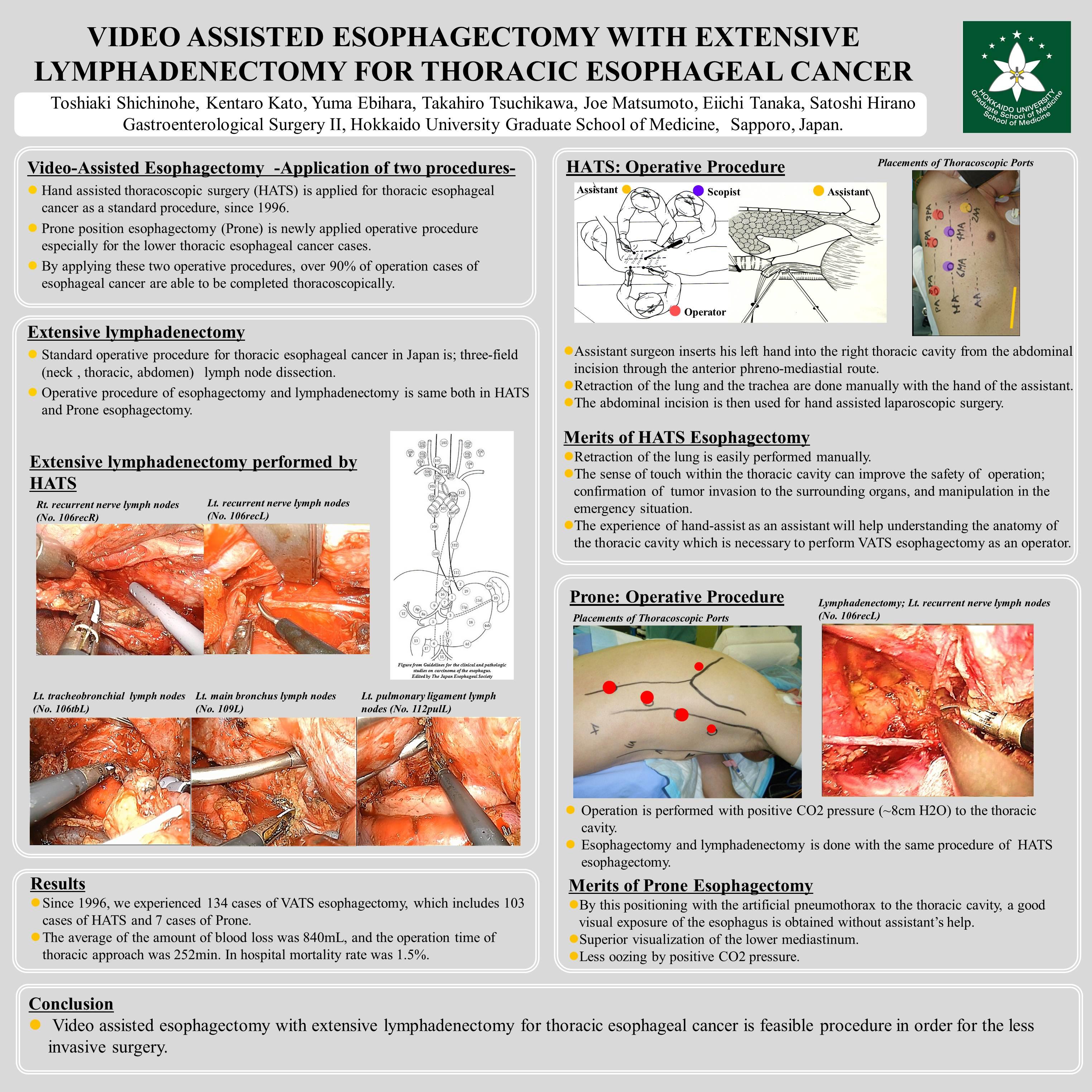
To accomplish extensive lymphadenectomy of paraesophageal and paratracheal lymph nodes as well as esophageal removal, we apply two different operation procedures; Hand assisted thoracoscopic surgery (HATS) is our standard procedure for thoracic esophageal cancer which is substitute for conventional open thoracotomy; Prone position esophagectomy (Prone) is newly applied operative procedure especially for the lower thoracic esophageal cancer cases. By applying these two operative procedures, over 90% of operation cases of esophageal cancer are able to be completed thoracoscopically.
Methods and procedures
VATS three-stage esophagectomy with extensive lymphadenectomy was performed by HATS or Prone procedure with gastric tube reconstruction and the cervical anastomosis.
HATS: The left lateral decubitus position is used for HATS. Assistant surgeon inserts his left hand into the right thoracic cavity from the abdominal incision through the anterior phreno-mediastial route. Retraction of the lung and trachea are thus done manually with the hand of the assistant. The abdominal incision is then used for hand assisted laparoscopic surgery (HALS).
The advantage of HATS is the gentle retraction of the lung from the caudal side of the thorax, thus obviating the need for lung retractors. Furthermore, this procedure allows the surgeon’s hand to use its sense of touch within the thoracic cavity, which can also confirm whether or not the tumor has invaded the surrounding organs such as the trachea.
Prone: Patient placed by the prone position. By this positioning with positive CO2 pressure to the thoracic cavity, the right lung falls away from the operative field both by gravity and the artificial pneumothorax, a good visual exposure of the esophagus without assistant’s help.
The advantage of this procedure is the superior visualization of the lower mediastinum. Thus, lower esophageal cancer case is the good applicant for this operation.
Results
Since 1996, we experienced 134 cases of VATS esophagectomy, which includes 103 cases of HATS and 7 cases of Prone.
The average of the amount of blood loss was 840mL, and the operation time of thoracic approach was 252min. In hospital mortality rate was 1.5%.
Conclusion
Video assisted esophagectomy with extensive lymphadenectomy for thoracic esophageal cancer is feasible procedure in term of the less invasive surgery.
Session Number: Poster – Poster Presentations
Program Number: P543
View Poster