David Y Lee, MD, Ronald Ross, MBBS, Michael Wassef, MD, Jun Levine, MD, Julio Teixeira, MD. St. Luke’s Roosevelt Hospital
Introduction
Single-port laparoscopy is a relatively new modality in abdominal surgery which offers improved cosmesis. Although studies to date have not been able to demonstrate that single-port laparoscopy achieves superior outcomes for postoperative pain compared to the conventional multiport technique, the single port technique may be more amenable to regional anesthetic interventions. In this pilot study, we evaluated the analgesic utility of Transversus Abdominal Plane (TAP) block in patients undergoing laparoscopic single-port sleeve gastrectomy (SPSG).
Methods
All patients undergoing laparoscopic sleeve gastrectomy were followed prospectively to evaluate postoperative pain utilizing the Visual Analog Scale (VAS). Patients received Patient-Controlled Analgesia (PCA) with intravenous hydromorphone postoperatively. Patients with VAS score >3 during the first 60 minutes postoperatively were offered a bilateral ultrasound-guided TAP block (2 x 30 ml of 0.2 % ropivacaine). The resulting VAS scores, opioid usage, and length of stay (LOS) were compared between patients who underwent SPSG that did and did not accept the TAP block, and patients who underwent multiport sleeve gastrectomy (MPSG).
Results
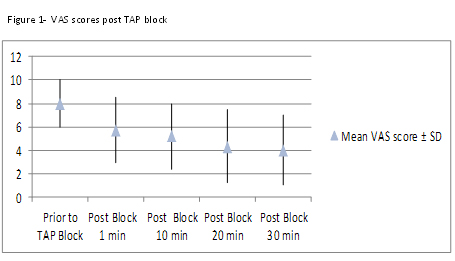
Within 30 minutes of administration, the mean pain score of patients receiving the TAP block decreased from 8.0 to 4.0 (p=0.037) (Figure 1). These patients also had the lowest average pain scores at all time points compared to other groups. This reached statistical significance at postoperative hours 1 and 12 (Table 1). Overall opioid usage and LOS were lower for patients who underwent SPSG versus MPSG but this did not reach statistical significance in our preliminary series. Administration of TAP blocks required 5-10 minutes of intervention time and was not associated with any complications.
Conclusion
Administration of TAP block significantly decreases postoperative the pain up to 12 hours after SPSG. Ultrasound guidance allowed for a reproducible and time-efficient analgesic benefit in the bariatric population. The combination of a single-port laparoscopic operation with TAP block may enhance postoperative pain control due to the block’s efficacy in covering the dermatomal distribution of the mid-abdomen. Future studies should evaluate the impact of preoperative administration of the block.
| SPSG + TAP (n=10) | SPSG (n=25) | MPSG (n=13) | p-Value | |
| Mean Age (y) | 43.1 ± 11.8 | 46.8 ± 13.3 | 45.4 ± 12.9 | 0.739 |
|
Mean BMI (kg/m²) |
42.2 ± 3.9 | 47.1 ± 6.6 | 50.9 ± 15.4 | 0.106 |
| Mean postoperative pain score | ||||
| 0hr | 4.0 ± 3.6 | 2.6 ± 3.9 | 3.3 ± 4.2 | 0.638 |
| 1hr | 2.7 ± 2.4 | 3.6 ± 2.9 | 6.2 ± 2.1 | 0.004 |
| 6hr | 0.3 ± 1.0 | 1.8 ± 2.4 | 1.9 ± 2.3 | 0.156 |
| 12hr | 0.1 ± 0.3 | 1.2 ± 1.5 | 0.6 ± 1.0 | 0.038 |
| 24hr | 0.4 ± 1.3 | 0.6 ± 1.0 | 0.7 ± 1.7 | 0.844 |
| Mean dose of patient controlled anlgesia (mg hydromorphone) | 5.9 ± 2.3 | 5.6 ± 2.9 | 6.9 ± 2.2 | 0.393 |
| Mean duration of patient controlled analgesia (h) | 43.0 ± 9.3 | 43.0 ± 16.0 | 43.8 ± 6.5 | 0.985 |
| Mean legnth of stay (h) | 56.3 ± 6.6 |
59.1 ± 17.1 |
65.0 ± 16.9 | 0.790 |
Session Number: Poster – Poster Presentations
Program Number: P419
View Poster