Madhu Ragupathi, MD, Dominique Vande Maele, MD, Javier Nieto, MD, T. Bartley Pickron, MD, Eric M Haas, MD FACS FASCRS. 1. Colorectal Surgical Associates, Ltd LLP, Houston, TX; 2. Division of Elective General Surgery, Department of Surgery, The University of Texas Medical School at Houston, TX
Introduction: Transanal endoscopic video-assisted (TEVA) excision represents an alternative approach for the surgical treatment of middle and upper rectal lesions not amenable to colonoscopic removal. By utilizing principles of single-incision laparoscopic surgery, TEVA excision optimizes access for safe and complete removal of these lesions without the need for a formal rectal resection. We describe our technique for TEVA excision and our early outcomes with this novel minimally invasive surgical approach.
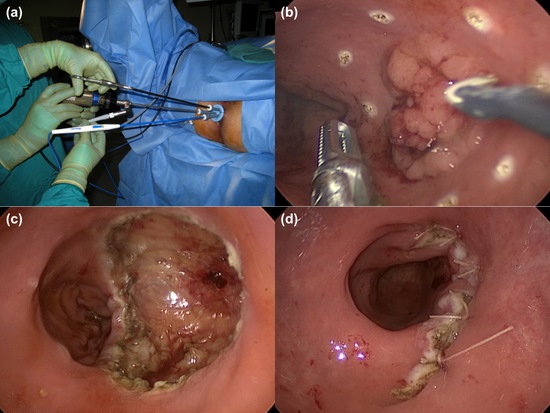
Methods and Procedures: Between March 2010 and September 2011, TEVA excision was performed for patients presenting for management of benign and malignant rectal lesions not amenable to colonoscopic or standard transanal removal. Patients were selected for TEVA excision if the proximal extent of the lesion extended beyond 8 cm from the anal verge. Early-stage adenocarcinomas (ultrasound stage: uT1N0) were also considered for TEVA excision. Demographic, intraoperative and postoperative data were assessed. A SILS™ port (Covidien, Mansfield, MA, USA) was placed in the anal canal for access in all cases (Fig. 1a). The port contains three cannulae for introduction of instrumentation into the rectal lumen and a supplementary cannula that facilitates carbon dioxide insufflation for creation of pneumorectum. Standard laparoscopic instruments were utilized for visualization, demarcation or scoring (Fig. 1b), and full-thickness transanal excision of the rectal lesion (Fig. 1c). The resulting wall defect was primarily closed with interrupted intra-luminal sutures (Fig. 1d).
Results: Twenty patients (50% male) with a mean age of 64.6±10.9 years (range: 40-86 years), mean BMI of 28.4±4.9 kg/m2 (range: 20.2-39.0 kg/m2), and median ASA of 2 (range: 1-3) underwent TEVA excision. Fourteen patients (70%) presented with benign disease (adenomas) and six patients (30%) presented with malignant disease (adenocarcinomas or carcinoids). The mean size of the lesions was 3.0±1.4 cm (range: 1.3-5.5 cm) and the mean distance from the anal verge was 10.6±2.4 cm (range: 6-15 cm). All TEVA excisions were successfully completed with a mean operative time of 80.1±21.0 min (range: 45-112 min). There were no intraoperative complications or conversions to another surgical approach. The mean length of hospital stay was 1.1±0.7 days (range: 0-3 days). One postoperative complication (5%) was encountered; a patient developed a rectovaginal fistula that spontaneously resolved without further intervention. Two patients (10%) underwent repeat interval TEVA excision, one for close surgical margins (within 1 mm) in a malignant case and another for recurrence of a villous adenoma 7 months after the initial procedure. One patient underwent a formal oncologic low anterior resection after TEVA excision revealed a T2 lesion.
Conclusions: Transanal endoscopic video-assisted excision is a safe and feasible approach for local excision of benign and superficial malignant rectal lesions. The approach facilitates exposure and access to pathologies of the middle and upper rectum and averts the need for formal rectal resection. Continued investigation and development of this novel and innovative modality will be important in establishing its role in minimally invasive colorectal surgery.
Session Number: PDIST – Posters of Distinction
Program Number: P003
View Poster