Koji Ikeda10, Yuji Nihisizawa10, Ichiro Takemasa1, Shuji Kitashiro2, Atsushi Nishimura3, Yoshiharu Sakai4, Junji Okuda5, Shintaro Akamoto6, Yusuke Kinugasa7, Tsunekazu Hanai8, Shinji Ohki9, Masaaki Ito10. 1Department of Surgery, Gastroenterological Surgery, Osaka University, 2Department of Surgery, Sapporo Tonan Hospital KKR Medical Center, 3Department of Surgery, Institute of Gastroenterology, Nagaoka Chuo General Hospital, 4Department of Surgery, Graduate School of Medicine, Kyoto University, 5Department of General and Gastroenterological Surgery, Cancer Center, Osaka Medical College, 6Department of Gastroenterological Surgery, Faculty of Medicine, Kagawa University, 7Divisions of Colon and Rectal Surgery, Shizuoka Cancer Center Hospital, 8Gastrointestinal Surgery, Department of Surgery, Fujita Health University School of Medicine, 9Department of Organ Regulatory Surgery, Fukushima Medical University, 10Division of Surgical Oncology, National Cancer Center Hospital East
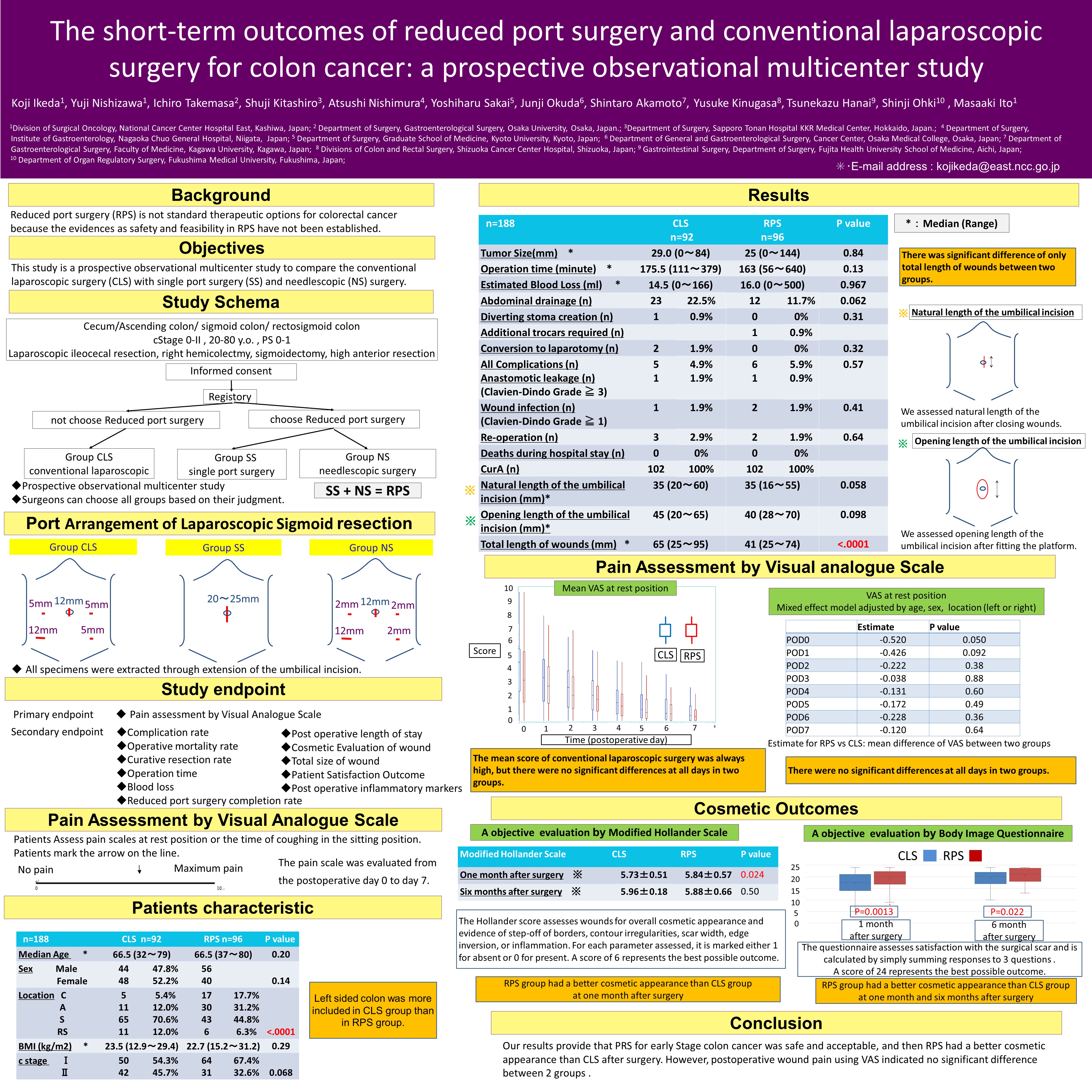
Objective: Reduced port surgery (RPS) is not standard therapeutic options for colorectal cancer because the evidences as safety and feasibility in RPS have not been established. This study is a prospective observational multicenter study to compare the conventional laparoscopic surgery (CLS) with single port surgery and needlescopic surgery.
Material and Methods: This study was multicenter trial conducted by 10 Japanese institutes between May 2013 and July 2015. We analyzed all the included patients with colon cancer of Stage I or II who had been treated with curative intent. Tumor location was assigned as right colon (cecum and ascending colon) or left colon (descending colon to rectosigmoid). The primary endpoint was pain assessment by Visual Analogue Scale (VAS). The pain scale was evaluated from the postoperative day 0 to day 7.
Results: A total of 188 consecutive patient records were available for analysis: 92 for CLS group and 96 for RPS group which included 46 with needlescopic surgery and 50 with single port surgery. CLS group included 44 males, 48 females (mean age, 63.4 ± 10.3 years); RPS group included 56 males, 40 females (mean age, 65.6 ± 9.3years). There were no significant differences of clinical backgrounds such as age, gender, BMI, clinical stage and size between two groups. Left sided colon was more included in CLS group than in RPS group (p<0.0001). There were no significant differences in operation time, blood loss, surgery-related complications with CTCAE grade 3-4 between two groups. The conversion rate was 2.0% in CLA group and none in RPS group. The reoperation rate was 2.9% in CLA group and 1.9% in RPS group, which was mainly due to anastomotic leakage. The overall hospital mortality rate was 0% and all the surgeries were with curative contents. Postoperative pain scores from 0 POD to 7 POD were no significant difference between two groups with mixed effect model adjusted be age, sex and tumor location (left side or right side).
Conclusions: Our results provide that PRS for colon cancer is safe and acceptable, but postoperative wound pain using VAS indicated no significant difference between RPS group and CLS group.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 79089
Program Number: P239
Presentation Session: Poster (Non CME)
Presentation Type: Poster