Renee Huang, MD, Cynthia Sulzbach, BS, Dominique McKeever, BA, Daniel Benchimol*, MD, FACS, John Marks, MD, FACS, FASCRS
Section of Colorectal Surgery, Lankenau Medical Center, Wynnewood, PA, United States, *Universite de Nice
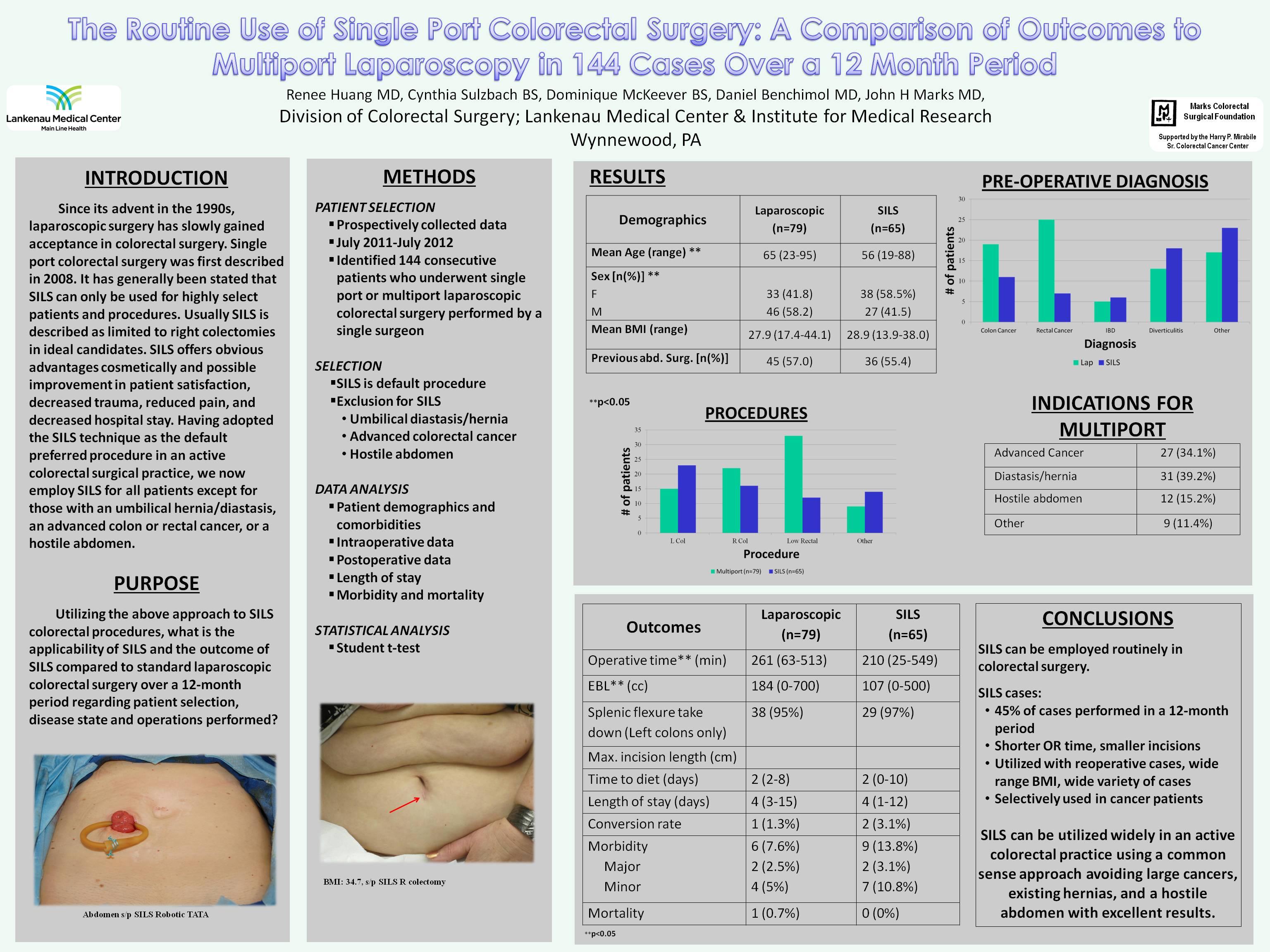
Introduction: The role of single-port colorectal surgery has been questioned except in highly select patients and procedures. This study analyzes short-term outcomes of the routine use of single-port surgery vs. standard laparoscopic colorectal surgery.
Methods: All laparoscopic colorectal procedures performed from July 2011 to July 2012 were identified from a prospectively maintained database. A retrospective analysis of 105 pre/peri/post-operative data points comparing single-port and multiport laparoscopic cases was performed. Single-port was performed preferentially for everything except rectal cancer. Indications for standard laparoscopy: umbilical hernia/diastasis (n=31); difficult pelvis (n=24); large inflammatory mass (n=10); unclear anatomy (n=5); advanced cancer (n=4); other (n=5). We compared demographics and outcomes of the two groups using a student t-test.
Results: Over 12 months, 144 patients underwent laparoscopic colorectal surgery by a single surgeon. Surgery was single-port in 65 patients (45%) and laparoscopic in 79 patients. The single-port group had more females (58.5% vs. 41.8%, p=0.04), was younger, mean age: 56 (19-88 y.o.) vs. 65 (23-95 y.o.) (p=0.004), with no difference in BMI: 28.9 (13.9-38.0) vs. 27.9 (17.4-44.1); previous surgery: 55.4% vs. 57.0%; multiple surgeries: 16.9% vs. 16.5%; or ASA class II or III: 98.4% vs. 93.6% (p>0.05). Diagnoses and procedures are below.
| Lap, n=79 (%) | SILS, n=65 (%) | |
| Colon Cancer | 19 (24.0) | 11 (16.9) |
| Rectal Cancer | 25 (31.6) | 7 (10.8) |
| IBD | 5 (6.4) | 6 (9.2) |
| Diverticulitis | 13 (16.5) | 18 (27.7) |
| Other | 17 (21.5) | 23 (35.4) |
| Lap, n=79 (%) | SILS, n=65 (%) | |
| Left colectomy | 15 (18.9) | 23 (35.3) |
| Right colectomy | 22 (27.9) | 16 (24.6) |
| Low rectal | 33 (41.9) | 12 (18.4) |
| Other | 9 (11.4) | 14 (21.6) |
Mean operative times were shorter [210 min (20-513) vs. 261 (25-549) (p=0.004)] and EBL less [107 ml (0-500) vs. 184 (0-700) (p=0.0002)] in single-port vs. laparoscopic. In subset analysis of left colons: 198.2 minutes (117-331) vs. 243 minutes (148-434) (p=0.08) and 108.1 ml (25-500) vs. 215.7 ml (25-650) (p=0.018); and in right colons: 148.5 minutes (79-296) vs. 172.9 minutes (107-277) (p=0.19) and 56.6 ml (20-200) vs. 123.2 ml (25-500) (p=0.0001). Splenic flexure was taken down 96% of the time in both groups. There were no conversions to open. Laparoscopy had one conversion to HALS (1.3%) and in two patients with single-port additional ports were placed (3.1%). Size of largest incision was smaller in the single-port group: 3.0 vs. 4.2 cm (p=0.0014). No differences existed in narcotic usage, time to flatus, BM, diet and discharge. Morbidity rate was the same: 13.8% single-port patients vs. 19.0% laparoscopic patients, with one anastomotic leak in the laparoscopic group. There was one (0.7%) mortality, and it occurred in the laparoscopic group.
Conclusion: Routine use of single-port surgery in a busy colorectal practice can be employed and should be considered. This study demonstrates in a wide spread of diagnoses and procedures that single-port surgery is a safe form of laparoscopic colorectal surgery and with a common sense approach can be widely used with slightly shorter operative times, less blood loss, and smaller incisions.
Session: Poster Presentation
Program Number: P071