Vinay Bajaj, MD, Anthony Dippolito, MD. Easton Hospital
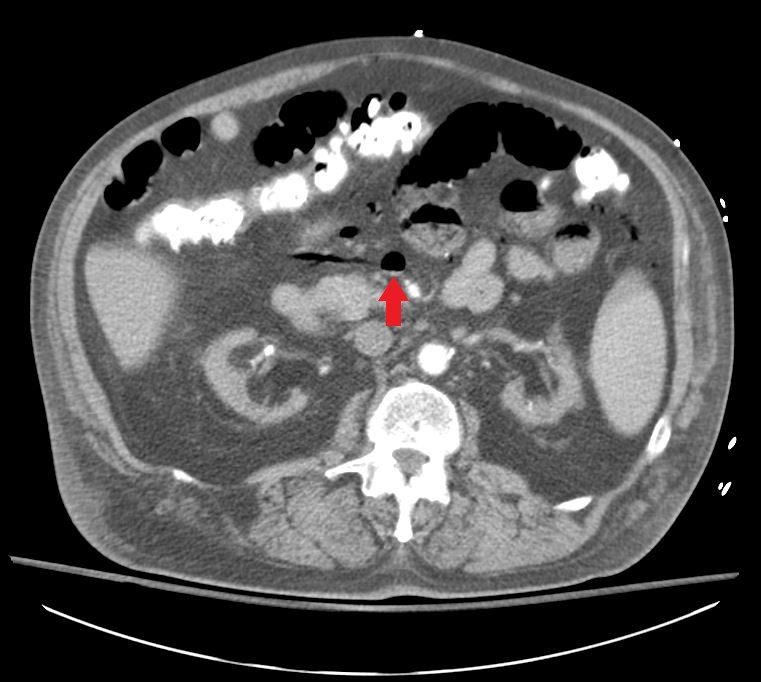
Our patient is a 67 year old male with significant history of insulin dependent diabetes, end stage renal disease on hemodialysis, cerebrovascular accident, and ischemic cardiomyopathy with EF 25% who was initially admitted for worsening dyspnea on exertion. He was found to be in flash pulmonary edema secondary to cardiogenic shock, and was being treated for the same. During his recovery patient started complaining of new onset 10/10 abdominal pain after his morning dialysis session, and was sent for a CT scan of his abdomen. On examining the patient he complained of no tenderness to palpation, no rebound or guarding, but returned to fetal position as soon as the exam was completed. Lab findings revealed a type II MI, with Troponin level of 1.66 and a lactic acidosis of 2.9. CT showed massive portovenous gas (PVG) with an impressive air fluid level in the mesenteric veins as shown below. At this point the patient was rushed to the operating room for an exploratory laparotomy that showed patchy dusky jejunal loop with a palpable and dopplerable superior mesenteric artery. At this point a decision to place an abthera vac was made with plans for a second look surgery within 24-48 hours.
Discussion: The presence of PVG on radiologic testing is usually considered a sign of impending doom. Factors that can cause this sign historically include, most commonly, bowel necrosis, ulcerative colitis intra-abdominal sepsis, small bowel obstruction, gastric ulcers, chronic obstructive pulmonary disease and even chronic steroid use in adults. The mortality rates vary from 56-90% based on the underlying etiology. Bowel ischemia, especially in adults, is especially morbid with rates from 75-90% cited in literature. The extent of bowel ischemia in the bowel wall is divided into three stages: Stage I: reversible ischemic enteritis limited to the mucosa; Stage II: necrosis of the mucosal and submucosal tissues, which may lead to fibrotic strictures; Stage III: the entire wall is affected by ischemia. PVG when associated with ischemia is usually related to Stage III and carries the highest mortality. Although CT scans are neither sensitive nor specific for the detection of bowel ischemia, the presence of PVG should raise concerns. Detection of air fluid levels in the pre-portal venous system as seen here could be an early indicator of the same, requiring emergent intervention to operate and concurrently to attempt to reverse the underlying etiology.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 91966
Program Number: P035
Presentation Session: Poster Session (Non CME)
Presentation Type: Poster