Objective: We describe our strategy and experience using the da Vinci S system to develop a completely robotic gastric bypass technique in a stepwise fashion.
The first robotic bariatric procedure was performed in1999 by Cardiere.1 The wristed movement and 7 degees of motion, enhanced high definition optics, superior ergonomics, and numerous other advantages have been previously described.2 Additionally, there has been a large case report showing a zero percent mortality and zero percent leak rate in over 500 robotic roux en Y gastric bypasses.3 Since the first robotic procedure, however, there has not been a significant application of robotic technology to bariatric procedures. Part of the slow adoption of robotic technology in bariatrics may be due to limitations in operating in multiple quadrants, lack of tactile feedback, and long operative times. These challenges may have contributed to the scarcity of totally robotic gastric bypass techniques. Hybrid techniques, in which portions of the procedure are completed robotically and portions are completed laparoscopically, have had little appeal to most bariatric surgeons.
Methods: In January of 2009 a single surgeon at Celebration Health started performing robotic gastric bypasses. The procedure was divided into segments: docking, creating the gastric pouch, creating the roux and biliopancreatic limbs and jejuno-jejunostomy, and creating the gastro-jejunostomy.
Each procedure is performed in the sequence listed above. The alimentary limb is created in an ante-colic, ante-gastric fashion. The jejuno-jejunostomy is formed by a stapled side to side anastamosis with closure of the resulting enterotomy in a running two-layered sutured closure. The gastro-jejunostomy is formed as a two-layered sutured anastamosis.Initial cases began laparoscopically with completion of the gastro-jejunostomy performed robotically. The jejuno-jejunostomy was added once the gastro-jejunosotomy was performed in 30 minutes or less. As proficiency increased in each step, we progressed to a totally robotic bypass procedure.
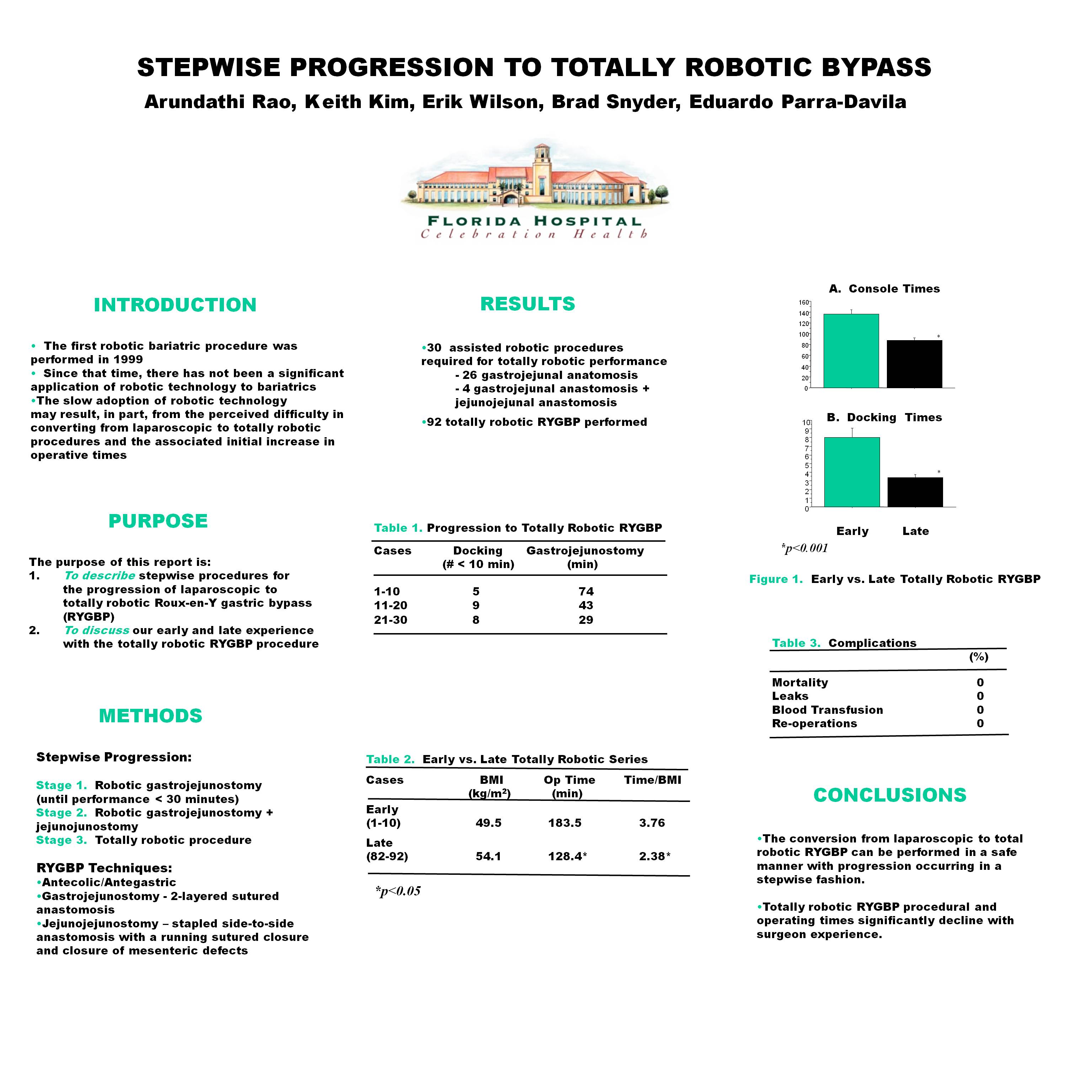
Results: Between January-July of 2009, thirty-six robotic assisted or totally robotic gastric bypasses were performed. A total of 26 gastro-jejeunal anastamosis, 4 gastro-jejunal anastamosis + jejuno-jejunal anastamosis and 6 totally robotic gastric bypass procedures were performed. The times for the completion of the gastro-jejunal anastamosis are listed below.
| Cases | Docking (cases under 10min/ total cases) | Gastro-jejunostomy(min) |
| 1-10 | 5/10 | 74 |
| 11-20 | 9/10 | 43 |
| 21-30 | 8/10 | 29 |
Six totally robotic cases were performed. Console time for the first case was 125 minutes. Cases 2-6 took an average of 106 minutes (range: 104-107 minutes). The gastro-jejunotomy was performed in an average of 24 minutes in these six cases.
Conclusions: The conversion from laparoscopic to totally robotic gastric bypass surgery can be achieved in a stepwise fashion to limit prolonged operative times over a relatively short experience.
1 GB Cadiere, et al., The world’s first obesity surgery performed by a surgeon at a distance. Obes Surg, 1999; 9(2): 206-209.
2 E Wilson. The Evolution of Robotic General Surgery. Scandanavian, Scan J Surg 2009;98:1-17.
3G. Hubens, et al., Roux-en-Y gastric Bypass procedure performed with the da Vinci Robot System: is it worth it? Surg. End .2008; 22(7): 1690-96.
Session: Poster
Program Number: P564