Sujata Sofat, MD, Ketan Patel, MD, Frank Albino, MD, Maurice Nahabedian, MD, Parag Bhanot, MD. Georgetown University Hospital Departments of General Surgery and Plastics Surgery
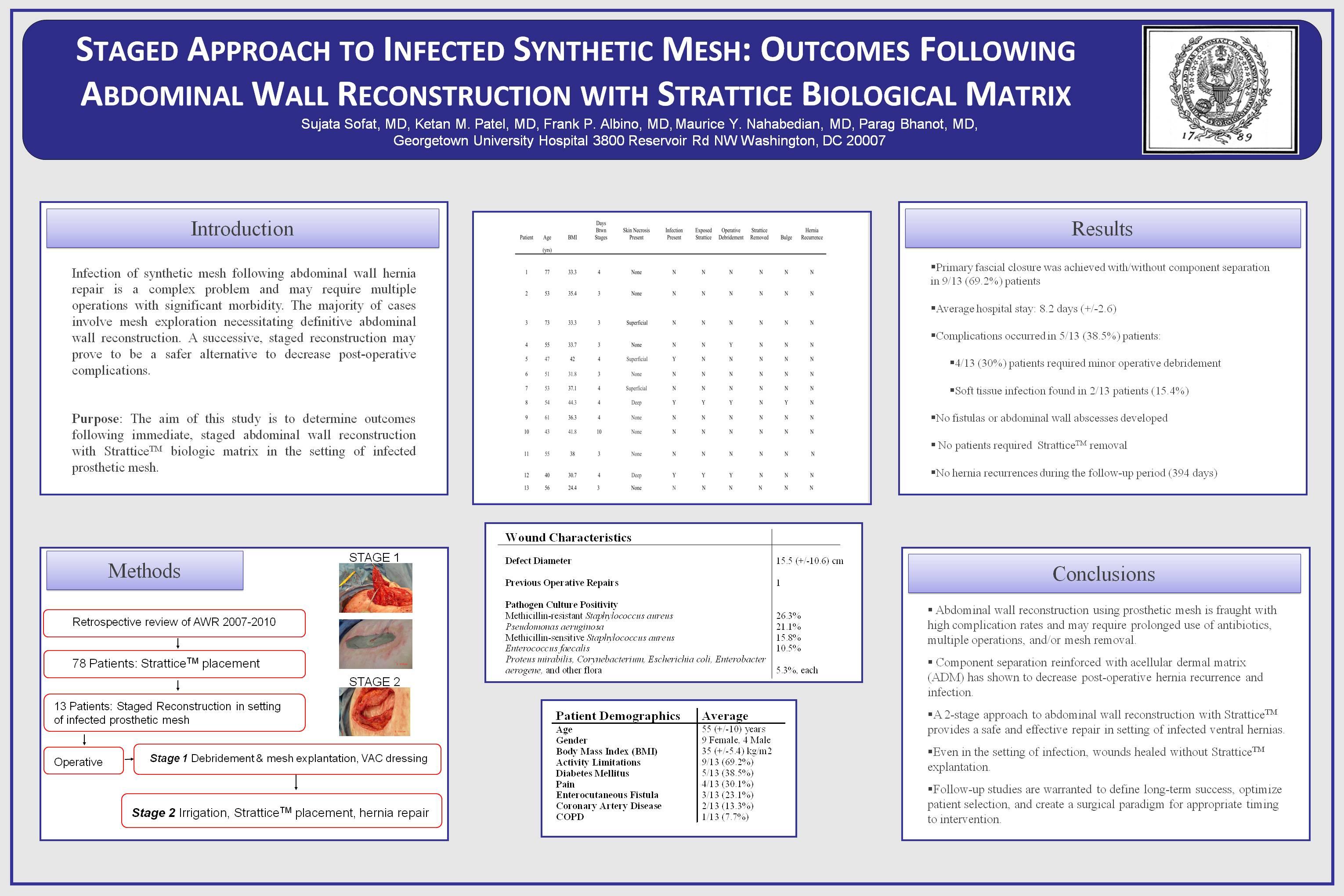
Background: Infection of synthetic mesh following abdominal wall hernia repair is a complex problem. Management can be difficult resulting in multiple operations with significant morbidity. The majority of cases involve mesh explantation necessitating definitive abdominal wall reconstruction. Strattice, a porcine-derived acellular dermal matrix, may provide a solution by providing a scaffold for native tissue regeneration and incorporation. Our study analyzed patients who had infected mesh requiring removal and placement of Strattice in a staged setting.
Methods: The authors performed a retrospective review of all patients who underwent complex AWR with Strattice placement by the senior author (P.B.) from 2007-2010 in the setting of infected mesh. Eligible patients presented with open wounds with infected mesh in the setting of previously repaired hernia with synthetic mesh. All patients underwent staged hernia repair; first stage was mesh explantation and debridement followed by VAC therapy/dressing changes. The second stage entailed formal hernia repair with Strattice reinforcement. Demographic, perioperative, and follow-up information were reviewed.
Results: 78 patients were identified as having Strattice implanted during the study period. 13 patients met the study criteria. Average patient age was 55 years with a BMI of 35.6. Average follow-up was 332.7 days. Co-morbidities include diabetes 5/13 (38.5%), coronary artery disease 2/15 (13.3%), and COPD 1/13 (7.7%). Recurrent/complex hernia was present in all patients. Mesh explantation occurred in all patients. Previous history of an enterocutaneous fistula was present in 3/13 (23.1%). Mean diameter of defect was 13.4cm. Pathogen culture positivity included MRSA (26.3%), Pseudomonas (21.1%), MSSA (15.8%), E. faecalis (10.5%), Proteus (5.3%), Corynebacterium (5.3%), E.coli (5.3%), and Enterobacter (5.3%). Average time between stages was 4 days. Primary fascial closure was achieved with/without component separation in 9/13 (69.2%) patients. Average hospital stay following repair was 8.2 days. Wound related complications occurred in 5/13 (38.5%) patients. Soft tissue infection with exposure of Strattice occurred in 2/13 (15.4%), but did not require removal. At an average of 4 weeks follow-up, all of the midline incisions had completely healed utilizing dressing changes and debridement when necessary.
Conclusion: Management of infected synthetic mesh is a challenging problem. A staged approach to abdominal wall reconstruction with Strattice appears to provide a safe and effective solution. Wound related complications do not require removal of Strattice limiting significant morbidity in these high-risk patients.
Session Number: Poster – Poster Presentations
Program Number: P277
View Poster