Maria S Altieri, Taher Gulamhusein, MD, Jie Yang, PhD, Andrew Bates, MD, Nabeel Obeid, MD, Jihye Park, MS, Mark Talamini, Aurora Pryor. Stony Brook Medical Center
Sleeve gastrectomy (SG) is the most commonly performed procedure for morbid obesity in the United States due to its technical ease and excellent weight loss. However, as it is a relatively new procedure, long term data is sparse. The purpose of our study was to evaluate emergency department (ED) visits and re-admission for the first year and rate of reoperation in the first three years following SG in New York State (NYS).
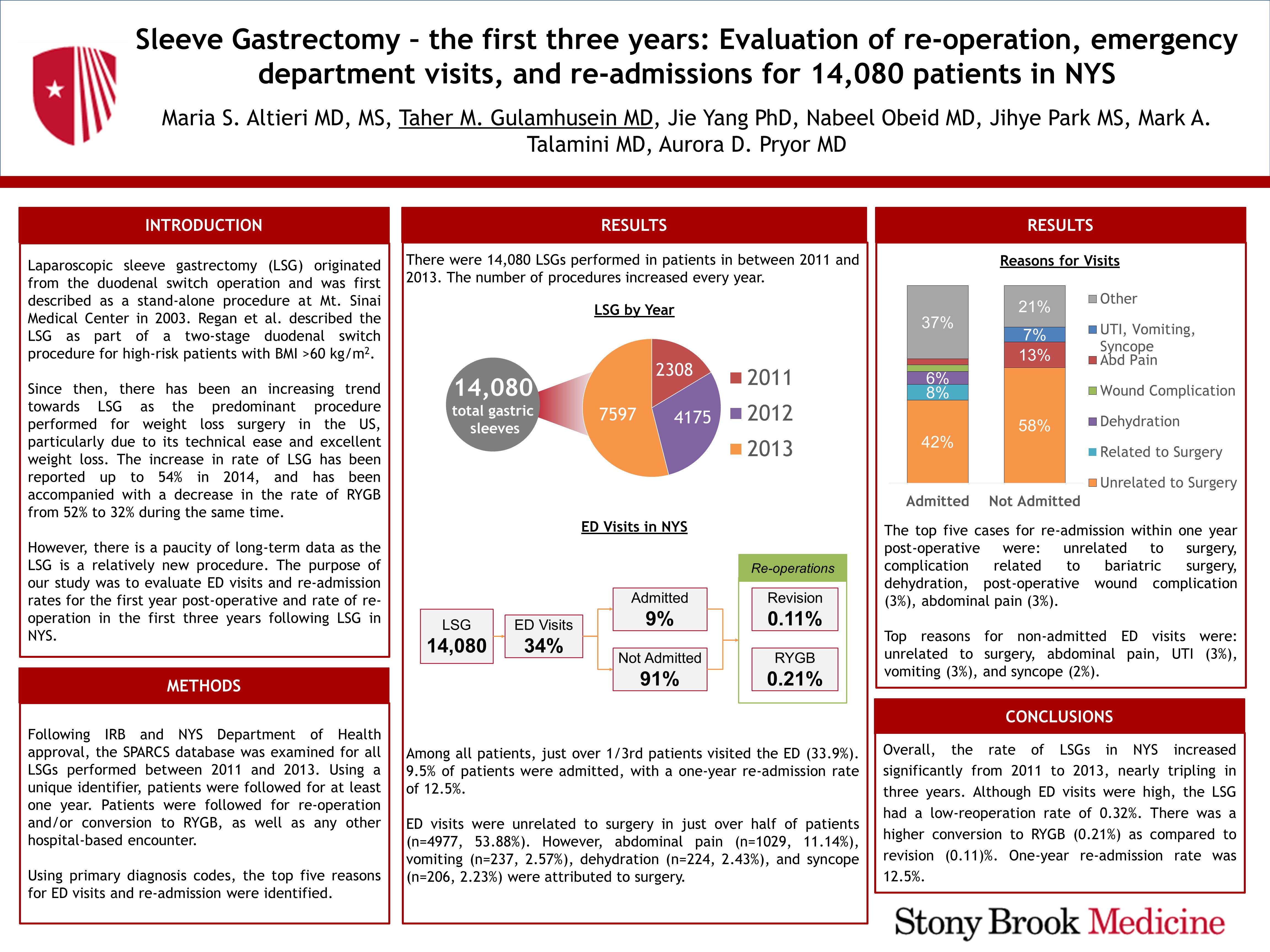
Following IRB and NYS Department of Health approval, the SPARCS database was examined for all SG procedures performed between 2011-2013. Using a unique identifier, patients were followed for at least one year to determine rate of re-operation and/or conversion to Roux-en-Y Gastric bypass (RYGB) as well as any other hospital-based encounter. The top five reasons for ED visits and readmission were identified. Chi-square tests with exact P-values based on Monte Carlo simulation were utilized to examine the marginal association between categorical variables. Welch’s t-test was used to compare marginal differences in the time interval between patients’ SG and any follow-up surgery according to different categorical variables.
Results: There were 14,080 SG performed in inpatients: 2,308 (16.3%) procedures in 2011, 4,175 (29.7%) in 2012, and 7,597 (54%) in 2013. Among all patients, just over 1/3 patients visited the ED (33.9%). One in ten (9.5%) of patients were admitted, with a 1-year readmission rate of 12.5%. ED visits were unrelated to surgery in just over half (n=4977,53.88%)). However, abdominal pain (n=1029,11.14%)), vomiting (n=237,2.57%), dehydration (n=224, 2.43%) and Syncope (n=206, 2.23%) were attributed to surgery. The top five causes for readmission with one-year post-operative were: unrelated to surgery (n=1101,41.74%), complication related to bariatric surgery (n=211 ,8%)), dehydration (n=171,6.48%), post-operative wound complications (n=89,3.37%), abdominal pain (n=78,2.96%). Top reasons for non-admitted ED visits were: unrelated to surgery (n=4328,58.26%), abdominal pain (n=957,12.88%), UTI (n=195, 2.62%), vomiting (n=189,2.54%), and syncope (n=170,2.29%). Overall, there is a low re-operation rate (0.32%), as conversion rate to RYBG and a revision of the sleeve were 0.21% and 0.11%, respectively. The average time to revision/conversion was 712+/-346.8 days. There were no patient specific factors predictive of revision, however, the revision rate was significantly different among different regions of operation.
Conclusion: The rate of SG procedures in NYS increased significantly during 2011-2013 (tripling in three years). Although ED visits were high, it had a low re-operation rate (0.32%), with higher conversion to RYGB compared to revision. One-year readmission rate was 12.5%.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 79842
Program Number: P013
Presentation Session: Poster of Distinction (Non CME)
Presentation Type: PDIST