Hiroyuki Kitagawa, MD, PhD, Tsutomu Namikawa, MD, PhD, Sunao Uemura, MD, Masaya Munekage, MD, Toyokazu Akimori, MD, PhD, Michiya Kobayashi*, MD, PhD, Kazuhiro Hanazaki, MD, PhD. Department of Surgery, Kochi Medical School; *Department of Human Health and Sciences, Kochi Medical School.
BACKGROUND: Thoracoscopic esophagectomy (TSE) for esophageal cancer has been spread as a less invasive surgery compared with conventional open thoracotomy approach. We have introduced the TSE in prone position since July 2009.
METHODS: Our procedure consists of three steps. The first step is neck dissection including lymph nodes around the recurrent nerve. The second step is TSE with mediastinal lymph nodes dissection. The third step was laparoscopic gastric mobilization and gastric tube formation followed the neck esophago-gastric tube anastomosis. We retrospectively reviewed 46 consecutive patients who underwent esophagectomy by TSE for esophageal cancer between July 2009 and July 2013 at Kochi Medical School to analyze the outcomes.
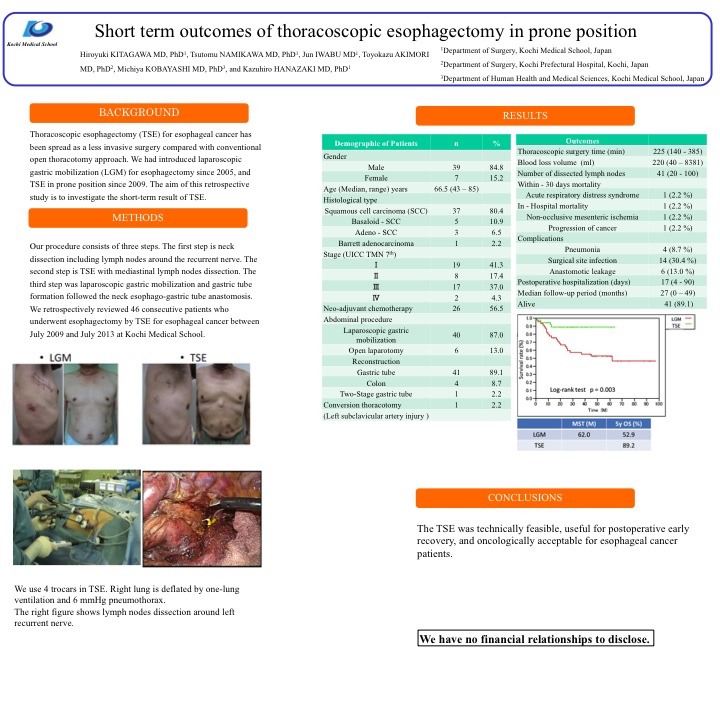
RESULTS: There were 39 (84.8 %) male and 7 (15.2 %) female. Median age was 66.5 (43 – 85) years old. In histological classification, 37 (80.4 %) cases were squamous cell carcinoma (SCC), 5 (10.9 %) were basaloid-SCC, 3 (6.5 %) were adeno-SCC, and the other 1 (2.2 %) was Barrett’s adenocarcinoma. According to UICC TNM 7th, 19 (41.3 %) cases were IA or IB, 8 (17.4 %) were IIA or IIB, 17 (37.0 %) were IIIA or IIIB or IIIC, and 2 (4.3 %) were IV. Neo-adjuvant chemotherapy was performed for 26 (56.5%) cases. In abdominal procedure, 40 (87.0 %) cases were performed laparoscopic gastric mobilization, 6 (13.0 %) were open laparotomy. Forty-one (89.1 %) cases were performed a gastric tube reconstruction, 4 (8.7 %) were colon, and 1 (2.2 %) was 2-stage reconstruction. One patient needed the open-conversion because of the left subclavicular artery injury. Median thoracoscopic surgery time was 225 (140 – 385) min, blood loss volume was 220 (40 – 8381) ml, and the number of dissected lymph nodes was 41 (20 – 100). Within 30 days mortality was observed in one patient (2.2 %), who died 4 days after the surgery caused by acute respiratory distress syndrome. Hospital mortality was observed in 2 patients (4.3 %). One patient died 35 days after the surgery due to non-occlusive mesenteric ischemia, the other one died 3 months after the surgery due to progression of cancer. In postoperative complications, pneumonia was observed in 4 (8.7 %) cases, surgical site infection was 14 (30.4 %) including 6 (13.0 %) of anastomotic leakage. Median length of postoperative hospitalization was 17 (4 – 90) days. Median follow-up period was 27 (0 – 49) months, and 41 (89.1 %) cases are alive.
CONCLUSIONS: The TSE was technically feasible, useful for postoperative early recovery, and oncologically acceptable for esophageal cancer patients.
View Poster