Christina A Del Pin, MD, FACS, Richard S Feinn, PhD, John Train, MD. Quinnipiac University/Frank H.Netter MD SOM.
Introduction: Right lower quadrant (RLQ) abdominal pain work-up for appendicitis (AP) has evolved from a wholly approach, to a more imaged based one. Delays in diagnosis due to non-diagnostic imaging, necessitating laparoscopy for critical treatment decisions, urges a revisit to the initial clinical presentation, diagnostic adjuncts and management of RLQ pain.
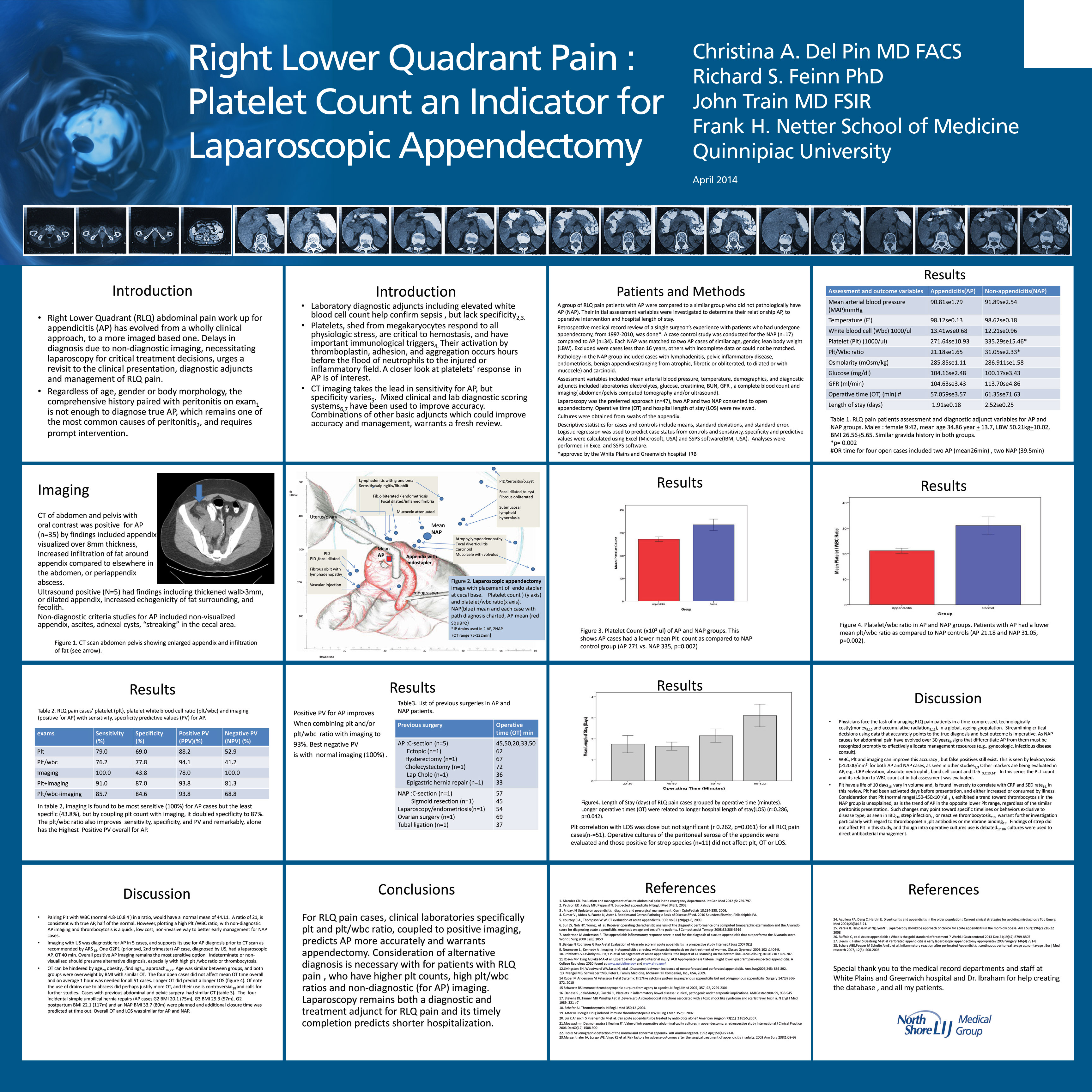
Methods: A retrospective case control study was conducted for RLQ pain patients, all of which had underwent appendectomy. Those negative for AP pathologically (NAP)(n=17) were compared to an AP control group (n=34), matched for age, gender, lean body weight, and were evaluated by logistic regression. NAP group included cases with lymphadenitis, pelvic inflammatory disease, endometriosis, benign appendices(ranging from atrophic, fibrotic , or obliterated, to dilated or with mucocele) and carcinoid. Variables included laboratories, imaging (ultrasound and computed tomography), OR time (OT) and length of stay (LOS). Laparoscopy was preferred approach (n=47), sensitivity, specificity and predictive values for AP were calculated.
Results: Imaging is most sensitive for appendicitis but the least specific. AP diagnosis in RLQ cases is related to a lower platelet count (plt) (NAP 335K, AP 271k p=0.002), and as well as a lower platelet: white blood cell ratio (plt/wbc) (NAP 31.05, AP 21.18, p=0.002). Using both plt and imaging results in logistic regression, sensitivity and specificity increased (from 79 to 91%, and 69 to 87%, respectively), as well as the predictive values (PV) ( seeTable1). Similarly, imaging and plt/wbc combination showed an increased sensitivity, specificity, PPV, NPV. Plt correlation with LOS was close (r=0.264) (p= 0.061) but not significant for all RLQ pain cases (n=51). Streptococcus+ peritoneal microbiology (n=11) did not affect Plt, OT, LOS. Longer OT was related to longer LOS (r= 0.286, p=0.042).
| exams | Sensitivity(%) | Specificity(%) | Positive PV(PPV)(%) | Negative PV (NPV)(%) |
| plt | 79.0 | 69.0 | 88.2 | 52.9 |
| plt/wbc | 76.2 | 77.8 | 94.1 | 41.2 |
| Imaging | 100.0 | 43.8 | 78.0 | 100.0 |
| plt+Imaging | 91.0 | 87.0 | 93.8 | 81.3 |
| plt/wbc+imaging | 85.7 | 84.6 | 93.8 | 68.8 |
Conclusions: For RLQ pain cases, clinical laboratories, specifically plt and plt/wbc ratio, coupled with positive imaging, predicts AP more accurately, and warrants appendectomy. Consideration of alternative diagnosis is necessary with RLQ pain cases having higher plt counts, high plt/WBC ratios and non-diagnostic imaging. Laparoscopy remains both a diagnostic and treatment adjunct for RLQ pain, and its timely completion predicts shorter hospitalization.
View Poster