Shinya Mikami, Tetsu Fukunaga, Hiroaki Itoh, Keizou Hataji, Ryuichi Oshima, Takeharu Enomoto, Jo Sakurai, Nobuyoshi Miyajima, Takehito Otsubo. St. Marianna University School of Medicine, Department of Gastroenterological and General Surgery,
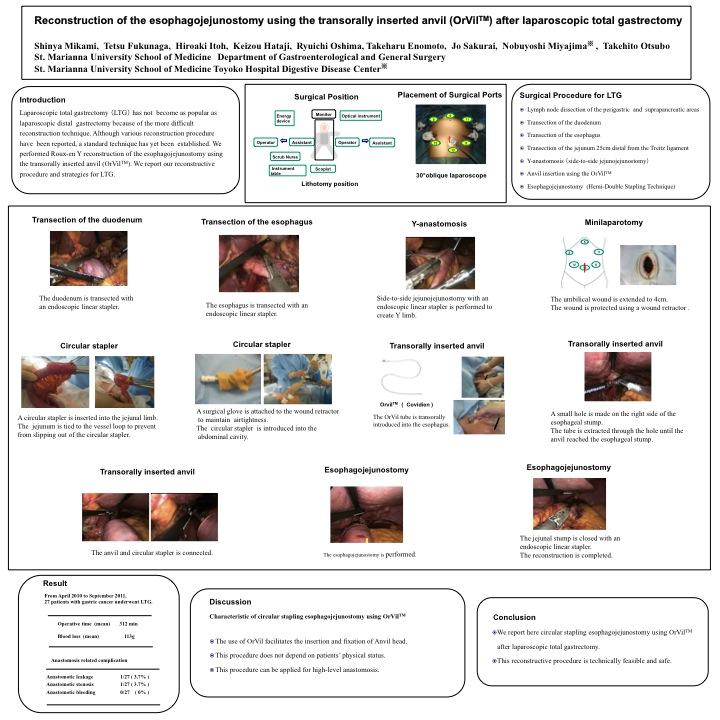
INTRODUCTION – Laparoscopic total gastrectomy (LTG) has not become as popular as laparoscopic distal gastrectomy because of the more difficult reconstruction technique. Although various reconstruction procedure have been reported, a standard technique has yet been established. As a reconstructive procedure after LTG, we perform Roux-en Y reconstruction of the esophagojejunostomy using the transorally inserted anvil (OrVilTM). We report our reconstructive procedure and strategies for LTG.
PROCEDURES – From April 2009 to September 2011, 27 patients with gastric cancer underwent LTG at our affiliated hospitals. The patient was placed in the supine position with the legs apart. A 30°oblique endoscope was inserted though the umbilical port, and a total of four ports inserted into the left upper, left flank, right upper and right flank quadrants. After Lymph node dissection of the perigastric and suprapancreatic areas, the duodenum was transected with an endoscopic linear stapler. The esophagus was transected with an endoscopic linear stapler. The jejunum 25cm distal from the Treitz ligament was transected with an endoscopic linear stapler. Side-to-side jejunojejunostomy with an endoscopic linear stapler was performed to prepare a Y limb. The umbilical wound was extended to 4cm. And, the jejunum limb was pulled out of the abdominal cavity. A circular stapler was inserted into the jejunal limb and fixed with the vessel loop. The circular stapler was introduced into the abdominal cavity. The OrVilTM tube was transorally introduced into the esophagus. A small hole was made on the right side of the esophageal stump. The tube was extracted through the hole until the anvil reached the esophageal stump. The tube was disconnected from the anvil by cutting the connecting thread and removed from the abdominal cavity. The anvil and circular stapler were connected and anastomosis was performed hemi-double stapling technique. The jejunal stump was closed with an endoscopic linear stapler.
RESULTS – The mean operative time for the 27 patients was 312 min, and the estimated blood loss was 113g. One patient who had anastomotic leakage at the esophagojejunostomy recovered by conservative treatment. Another patient who developed anastomosis stenosis was successfully treated by endoscopic balloon dilatation.
CONCLUSION – The circular stapling esophagojejunostomy using OrVilTM facilitates insertion and fixation of Anvil head. Also, this procedure does not depend on patients’ physical status and can be applied for high-level anastomosis.
Session Number: Poster – Poster Presentations
Program Number: P628
View Poster