K A Zuberi, MD, B R Zagol, MD, V K Narula, MD, V C Memark, MD, J B Anderson, MD, W Scott Melvin, MD, J W Hazey, MD. The Ohio State University Medical Center: Center for Minimally Invasive Surgery, Columbus, OH, USA
Introduction:
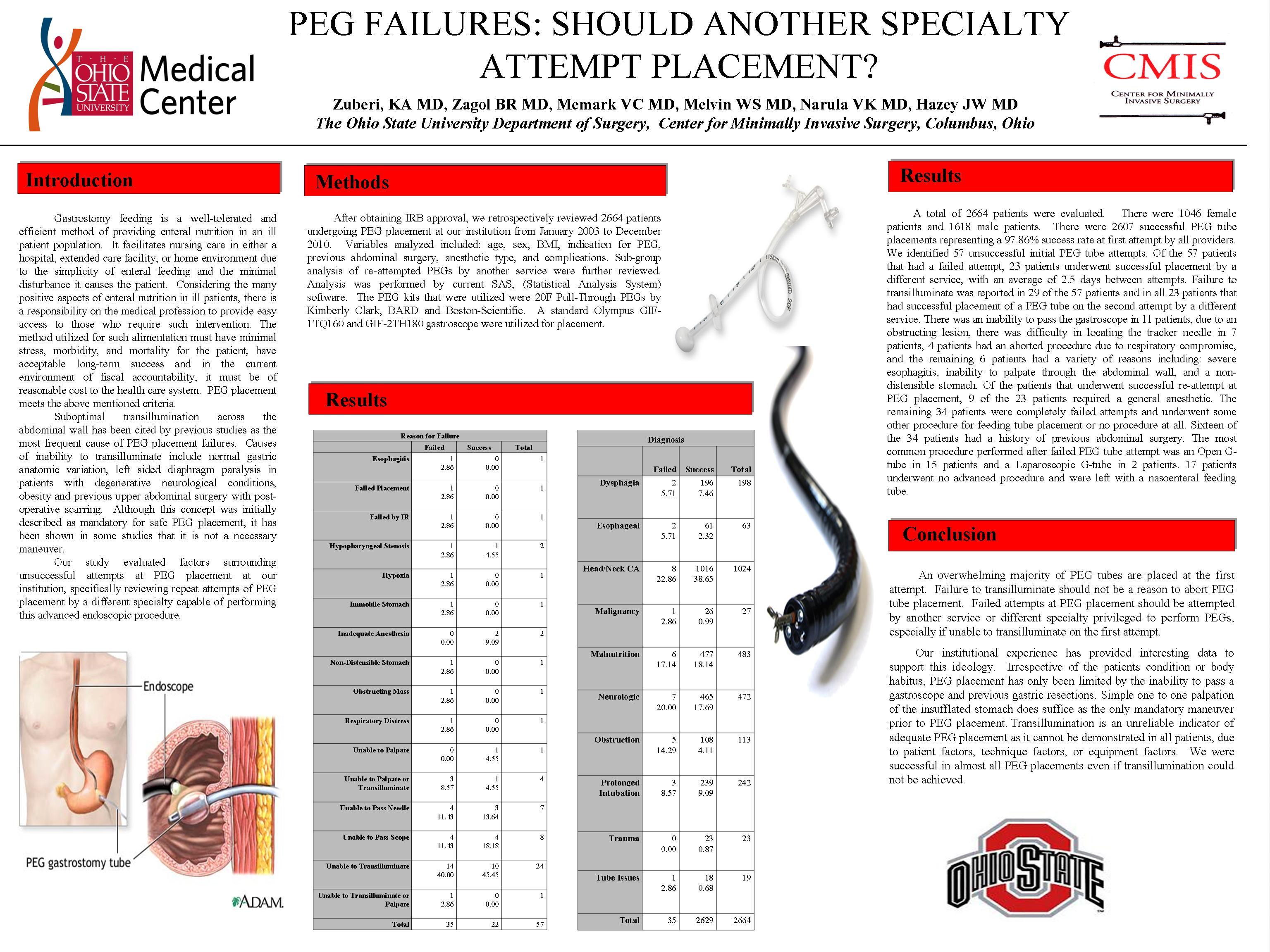
Percutaneous Endoscopic Gastrostomy (PEG) tube placement is the preferred enteral access for patients unable to swallow or with pre-existing or anticipated malnutrition. We evaluated factors surrounding unsuccessful attempts at PEG placement at our institution, specifically reviewing repeat attempts of tube placement by a different service.
Methods and Procedures:
We retrospectively reviewed 2664 patients undergoing PEG placement at our institution from January 2003 to December 2010. Variables analyzed included: age, sex, BMI, indication for PEG, previous abdominal surgery, anesthetic type, and complications. Sub-group analysis of re-attempted PEGs by another service, were further reviewed. Analysis was performed by current SAS, (Statistical Analysis System) software.
Results:
A total of 2664 patients were evaluated. There were 1046 female patients and 1618 male patients. There were 2607 successful PEG tube placements representing a 97.86% success rate at first attempt by all providers. We identified 57 unsuccessful initial PEG tube attempts. Of the 57 patients that had a failed attempt, 23 patients underwent successful placement by a different service, with an average of 2.5 days between attempts. Failure to transilluminate was reported in 29 of the 57 patients and in all 23 patients that had successful placement of a PEG tube on the second attempt by a different service. There was an inability to pass the gastroscope in 11 patients, due to an obstructing lesion, there was difficulty in locating the tracker needle in 7 patients, 4 patients had an aborted procedure due to respiratory compromise, and the remaining 6 patients had a variety of reasons including: severe esophagitis, inability to palpate through the abdominal wall, and a non-distensible stomach. Of the patients that underwent successful re-attempt at PEG placement, 9 of the 23 patients required a general anesthetic. The remaining 34 patients were completely failed attempts and underwent some other procedure for feeding tube placement or no procedure at all. Sixteen of the 34 patients had a history of previous abdominal surgery. The most common procedure performed after failed PEG tube attempt was an Open G-tube in 15 patients and a Laparoscopic G-tube in 2 patients. 17 patients underwent no advanced procedure and were left with a nasoenteral feeding tube.
Conclusion(s):
An overwhelming majority of PEG tubes are placed at the first attempt. Failure to transilluminate should not be a reason to abort PEG tube placement. Failed attempts at PEG placement should be attempted by another service or different specialty privileged to perform PEGs, especially if unable to transilluminate on the first attempt.
Session Number: Poster – Poster Presentations
Program Number: P633
View Poster