Tatsushi Suwa, MD, Satoshi Inose, MD, Tomoko Fukushima, MD, Kenta Kitamura, MD, Tomonori Matsumura, MD, Kazuhiro Karikomi, MD, Eishi Totsuka, MD, Motoi Koyama, MD, Keigo Okada, MD, Naokazu Nakamura, MD, Hiroyuki Suzuki, MD, Shigeru Masamura, MD. Kashiwa Kosei General Hospital
Introduction: Laparoscopic techniques in anti-reflux surgery for GERD patients are still considered complicated by many surgeons. We have simplified it and established our practical procedure.
Surgical Procedure:
Setting
Our 5-trocar setting with patients in the reverse Trendelenburg's position is as follows: 12 mm trocar just below the navel (A), 5 mm trocar at the upper right abdomen for pulling up lateral segment of the liver, 5 mm trocar at the upper right abdomen, 12 mm trocar at the upper left abdomen (B), 5 mm trocar at the middle left abdomen (C).
Step 1
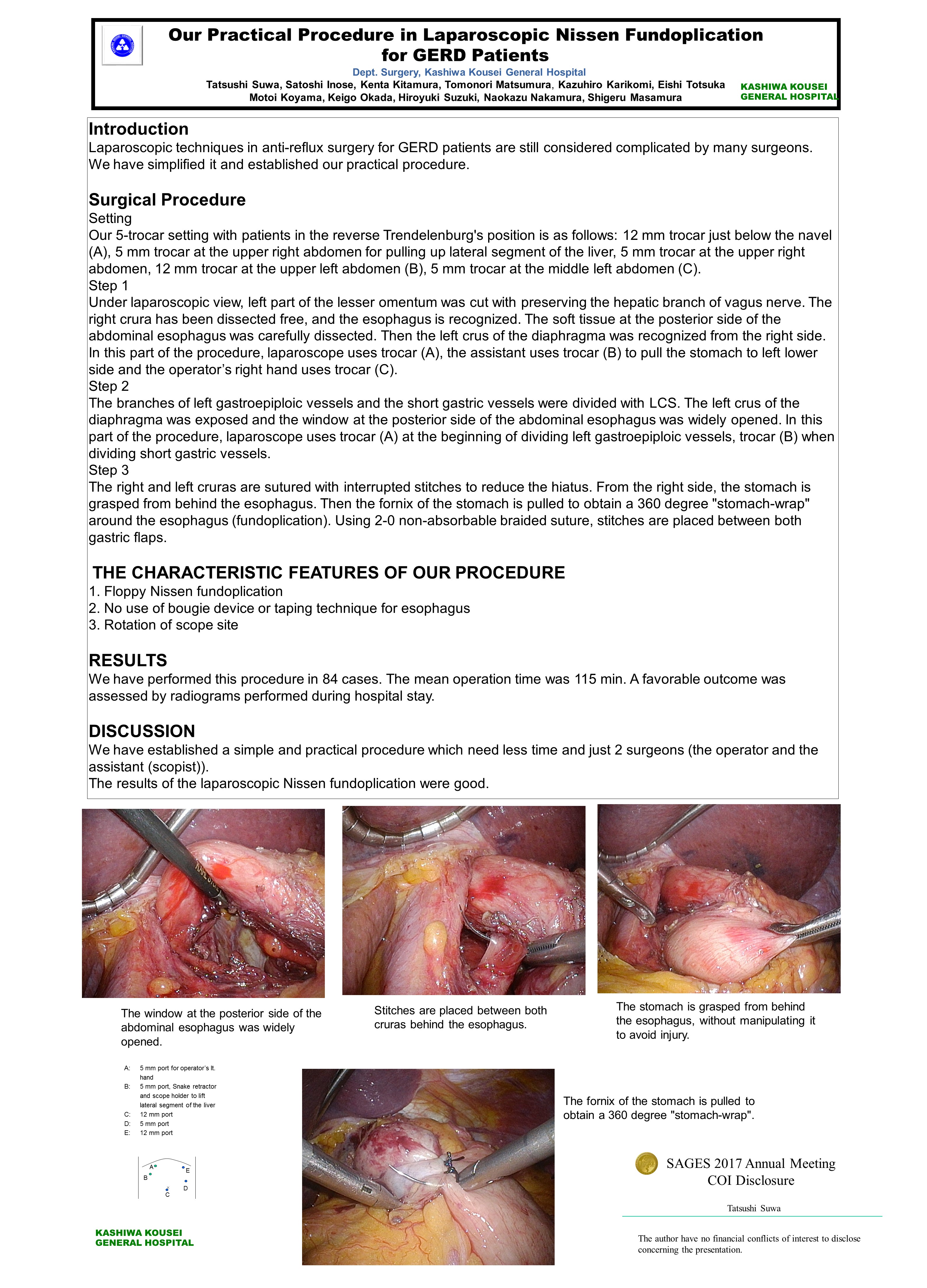
Under laparoscopic view, left part of the lesser omentum was cut with preserving the hepatic branch of vagus nerve. The right crura has been dissected free, and the esophagus is recognized. The soft tissue at the posterior side of the abdominal esophagus was carefully dissected. Then the left crus of the diaphragma was recognized from the right side. In this part of the procedure, laparoscope uses trocar (A), the assistant uses trocar (B) to pull the stomach to left lower side and the operator’s right hand uses trocar (C).
Step 2
The branches of left gastroepiploic vessels and the short gastric vessels were divided with LCS. The left crus of the diaphragma was exposed and the window at the posterior side of the abdominal esophagus was widely opened. In this part of the procedure, laparoscope uses trocar (A) at the beginning of dividing left gastroepiploic vessels, trocar (B) when dividing short gastric vessels.
Step 3
The right and left cruras are sutured with interrupted stitches to reduce the hiatus. From the right side, the stomach is grasped from behind the esophagus. Then the fornix of the stomach is pulled to obtain a 360 degree "stomach-wrap" around the esophagus (fundoplication). Using 2-0 non-absorbable braided suture, stitches are placed between both gastric flaps.
RESULTS:
We have performed this procedure in 84 cases. The mean operation time was 115 min. A favorable outcome was assessed by radiograms performed during hospital stay.
DISCUSSION:
We have established a simple and practical procedure which need less time and just 2 surgeons (the operator and the assistant (scopist)).
The results of the laparoscopic Nissen fundoplication were good.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 78600
Program Number: P392
Presentation Session: Poster (Non CME)
Presentation Type: Poster