Matt B Martin, MD, Ben T Hoxworth, MD, Kristen R Earle, MD, David H Newman, MD. Moses Cone Health Systems, Greensboro, NC 27401
Introduction LAGB with hiatus hernia repair may be a successful procedure for mechanical GER as well as obesity. Placement of a laparoscopic adjustable gastric band (LAGB) in a patient with an underlying sliding hiatus hernia usually results in weight loss failure since adequate restriction is accompanied by increasing nocturnal GER symptoms and thus weight loss is limited. Our bariatric team initially recommended laparoscopic gastric bypass for such patients. In 2008 after certain patients wanted a LAGB but had sliding hiatus hernias on UGI, we began repairing these hernias at the time of LAGB. This retrospective review examines the effectiveness of hiatus hernia repair when combined with LAGB in treating GER as a comorbidity of obesity. Repairing a mechanical defect is important in LABG success to permit adequate restriction without inducing severe GER.
Methods Since September 2008, our bariatric group has identified 52 patients with symptomatic GER or an identifiable anatomic defect who underwent LAGB and had concomitant hiatus hernia repair. This retrospective review seeks to identify the success rate of posterior crural repair with LAGB placement.
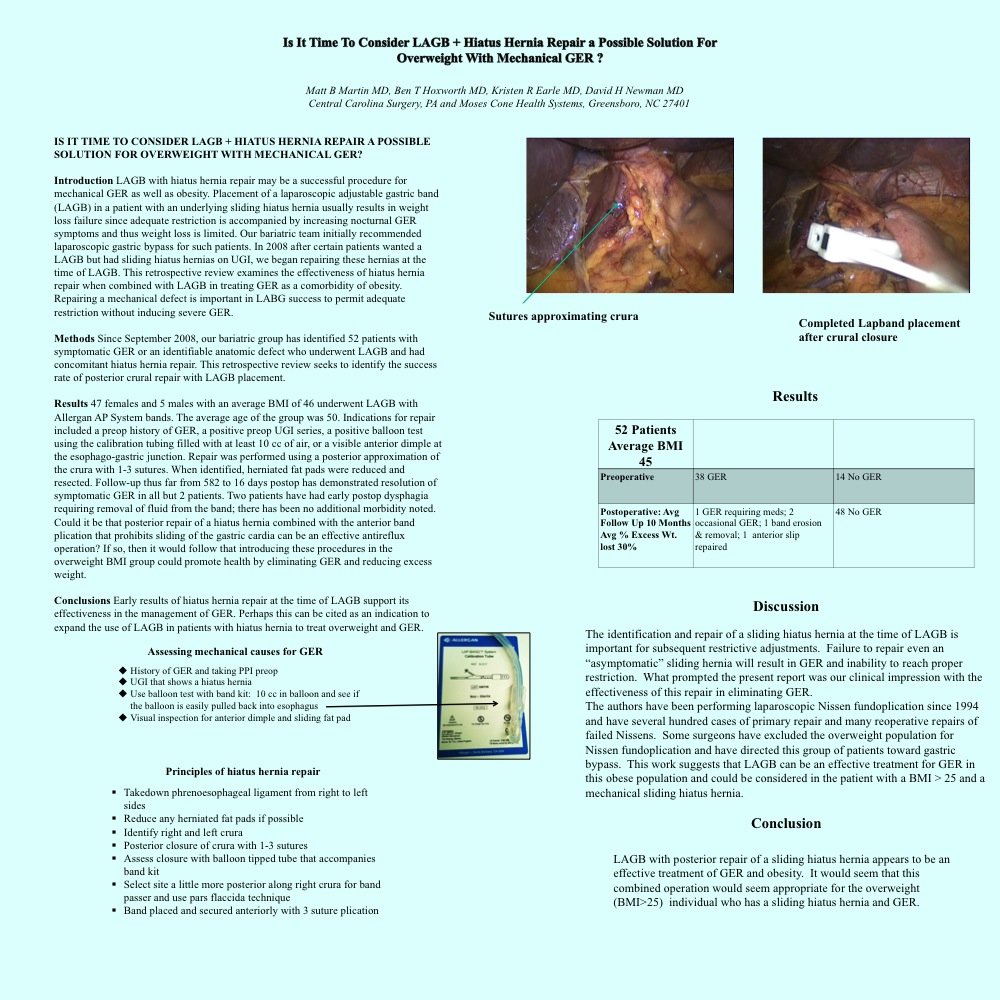
Results 47 females and 5 males with an average BMI of 46 underwent LAGB with Allergan AP System bands. The average age of the group was 50. Indications for repair included a preop history of GER, a positive preop UGI series, a positive balloon test using the calibration tubing filled with at least 10 cc of air, or a visible anterior dimple at the esophago-gastric junction. Repair was performed using a posterior approximation of the crura with 1-3 sutures. When identified, herniated fat pads were reduced and resected. Follow-up thus far from 582 to 16 days postop has demonstrated resolution of symptomatic GER in all but 2 patients. Two patients have had early postop dysphagia requiring removal of fluid from the band; there has been no additional morbidity noted. Could it be that posterior repair of a hiatus hernia combined with the anterior band plication that prohibits sliding of the gastric cardia can be an effective antireflux operation? If so, then it would follow that introducing these procedures in the overweight BMI group could promote health by eliminating GER and reducing excess weight.
Conclusions Early results of hiatus hernia repair at the time of LAGB support its effectiveness in the management of GER. Perhaps this can be cited as an indication to expand the use of LAGB in patients with hiatus hernia to treat overweight and GER.
Session: Poster
Program Number: P045
View Poster
{kind=link}