Ryo Shimoyama, MD, Masataka Ikeda, MD, Michihiko Miyazaki, MD, Takuya Hamakawa, MD, Sakae Maeda, MD, Mamoru Uemura, MD, Masakazu Miyake, MD, Naoki Hama, Kazuhiro Nishikawa, MD, Atsushi Miyamoto, MD, Motohiro Hirao, MD, Shoji Nakamori, MD, Mitsugu Sekimoto, MD. Osaka National Hospital
Background: The Wells type posterior rectopexy is one of the standard methods of choice for the treatment of rectal prolapse. Laparoscopic surgery has been shown to be feasible in this technique. We have introduced reduced port laparoscopic surgery (RPS) for rectal prolapse. The aim of this study was to evaluate the feasibility of RPS for Wells type posterior rectopexy.
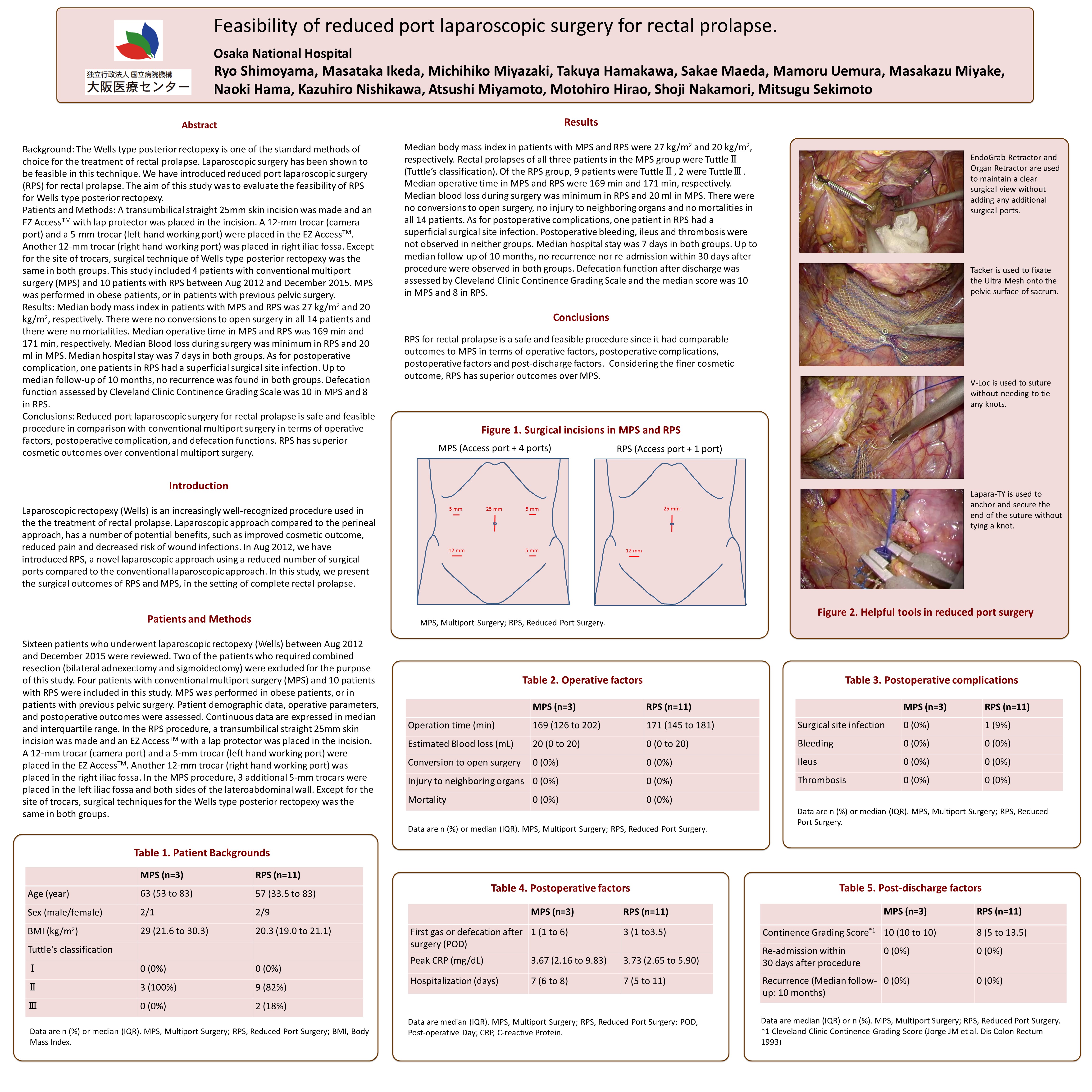
Patients and Methods: A transumbilical straight 25mm skin incision was made and an EZ AccessTM with lap protector was placed in the incision. A 12-mm trocar (camera port) and a 5-mm trocar (left hand working port) were placed in the EZ AccessTM. Another 12-mm trocar (right hand working port) was placed in right iliac fossa. Except for the site of trocars, surgical technique was same as the conventional multiport surgery (MPS). This study included 4 patients with MPS and 10 patients with RPS between Aug 2012 and December 2015. Twelve patients had rectal prolapse without anal prolapse (Tuttle type II), and 2 patients had intussusception of the rectum (Tuttle type III) and MPS was performed in obese patients, or in patients with previous pelvic surgery.
Results: Mean body mass index in patients with MPS and RPS was 27 kg/m2 and 20 kg/m2, respectively. There were no conversions to open surgery in all 14 patients and there were no mortalities. Mean operative time in the MPS group and RPS group were 169 min and 171 min, respectively. Blood loss during surgery was very slight amount in the RPS group and 20 ml in the MPS group. Mean postoperative hospital stay was 7 days in both groups. As for the postoperative complications, one patients in the RPS group had a superficial surgical site infection. Up to median follow-up of 10 months, no recurrence was found in both groups. Defecation function assessed by Cleveland Clinic Continence Grading Scale was 10 in the MPS group and 8 in the RPS group.
Conclusions: Reduced port laparoscopic surgery for rectal prolapse in selected patients is safe and feasible procedure in comparison with conventional multiport surgery in terms of operative factors, postoperative complication, and defecation functions. RPS has superior outcomes over conventional multiport surgery.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 78791
Program Number: P624
Presentation Session: Poster (Non CME)
Presentation Type: Poster