Hae Jung Son, MD, Dae Kyung Sohn, MD PhD, Chang Won Hong, MD, Kyung Su Han, MD, Byung Chang Kim, MD, Ji Won Park, MD, Hyo Seong Choi, MD PhD, Hee Jin Chang, MD PhD, Jae Hwan Oh, MD PhD. Center for Colorectal cancer, Research Institute and Hospital, National Cancer Center, Goyang, Gyeonggi, South Korea
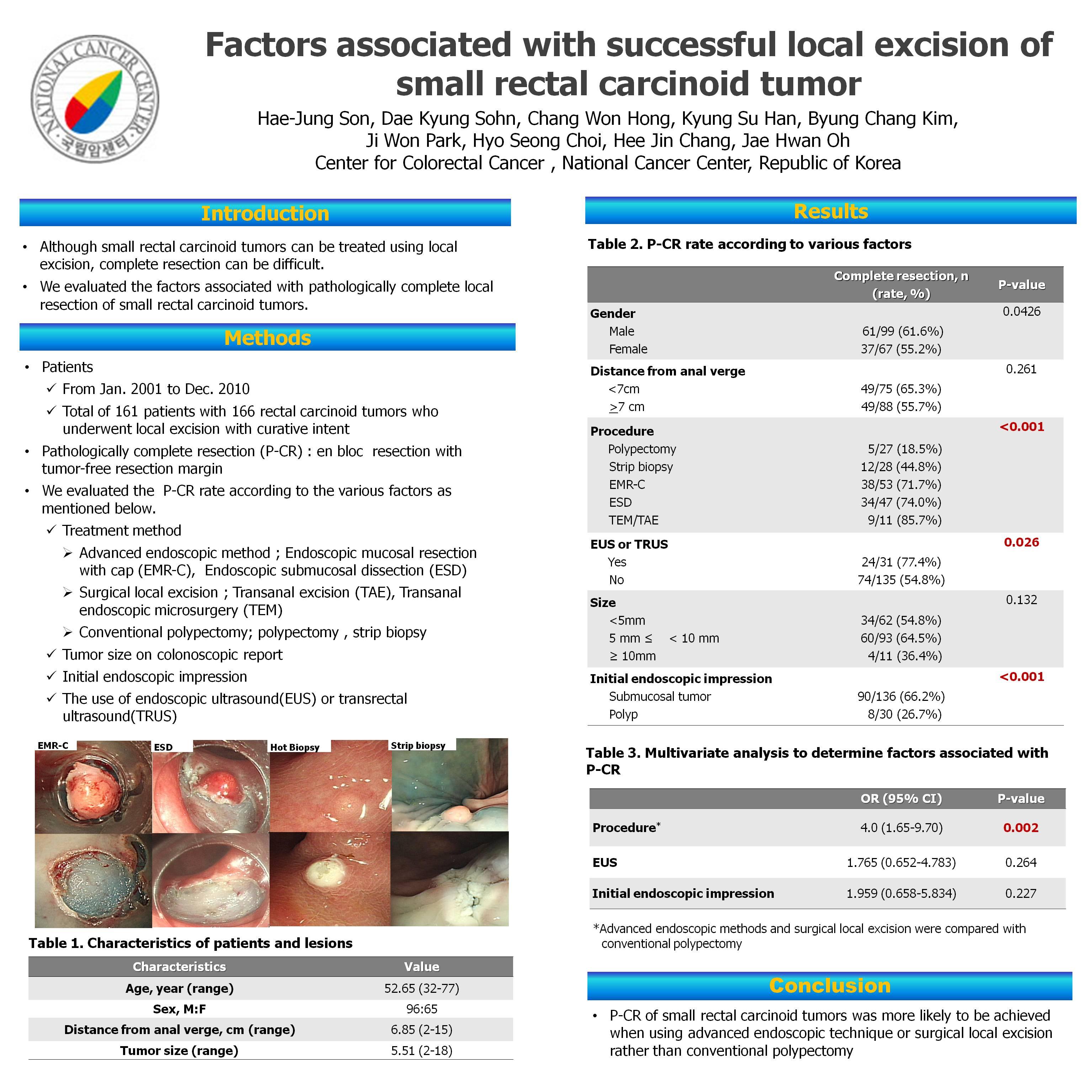
INTRODUCTION Small rectal carcinoid tumors can be treated by local excision, but complete resection may be difficult because tumors are located in the submucosal layer. We performed this study to find out the risk factors associated with pathologically complete resection of rectal carcinoid tumor.
METHODS AND PROCEDURES From January 2001 to December 2010, total 299 patients with colorectal carcinoid tumors were treated at the National Cancer Center, South Korea. Among of them, we excluded patients who had metastatic disease(n=10), who underewent radical operation(n=33), who were diagnosed in other hospitals(n=83) and who had colon carcinoid tumors(n=3). Finally, 170 patients with 175 rectal carcinoid tumors, who treated with local excision including endoscopic resection and surgical resection were enrolled this study. A pathologically complete resection(P-CR) was defined as an en bloc resection with tumor-free lateral and deep margin. Local treatment methods were classified to conventional polypectomy including strip biopsy, snare polypectomy and hot biopsy, advanced endoscopic techniques including endoscopic mucosal resection with cap(EMR-C) and endoscopic submucosal dissection(ESD) and surgical local excision including transanal excision(TAE) and transanal endoscopic microsurgery(TEM). We evaluated the P-CR rate according to treatment method, tumor size, endoscopically initial impression and use of endoscopic ultrasound(EUS) or transrectal ultrasound(TRUS).
RESULTS Mean size of tumors was 5.60 ± 2.41mm (range from 2mm to 18mm) and all lesions were confined to the submucosal layer. P-CR rate of all lesions was 60.6%. When endoscopic impression was submucosal tumor, P-CR rate increased to 68.1%. P-CR rates according to treatment methods were 31.6%, 73.1%, 85.7% in conventional polypectomy, advanced endoscopic technique, and surgical local excision, respectively. Because P-CR rates were not significantly different between advanced endoscopic technique and surgical local excision, we performed further analysis with two groups of treatment methods including conventional polypectomy and advanced endoscopic technique or surgical local excision. Univariate analysis showed that treatment method, use of EUS or TRUS and endoscopically initial impression were related to P-CR. On multivariate analysis, treatment method was the only factor associated with P-CR.
CONCLUSIONS Advanced endoscopic technique or surgical local excision was more beneficial to achieve pathologically complete resection than conventional polypectomy in local treatment of small rectal carcinoid tumors.
Session Number: Poster – Poster Presentations
Program Number: P069
View Poster