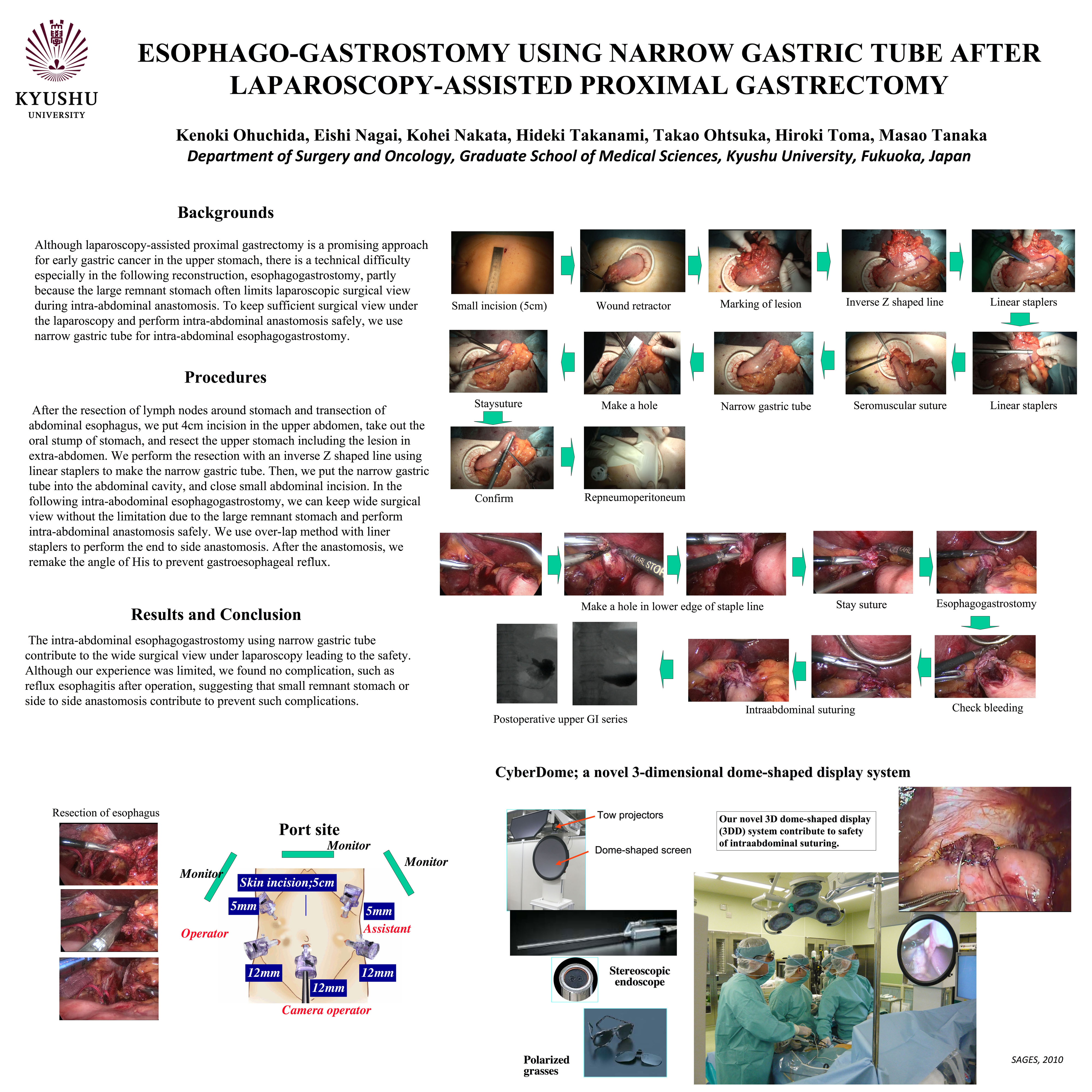
Introduction: Although laparoscopy-assisted proximal gastrectomy is a promising approach for early gastric cancer in the upper stomach, there is a technical difficulty especially in the following reconstruction, esophagogastrostomy, partly because the large remnant stomach often limits laparoscopic surgical view during intra-abdominal anastomosis. To keep sufficient surgical view under the laparoscopy and perform intra-abdominal anastomosis safely, we use narrow gastric tube for intra-abdominal esophagogastrostomy.
Procedures: After the resection of lymph nodes around stomach and transection of abdominal esophagus, we put 4cm incision in the upper abdomen, take out the oral stump of stomach, and resect the upper stomach including the lesion in extra-abdomen. We perform the resection with an inverse Z shaped line using linear staplers to make the narrow gastric tube. Then, we put the narrow gastric tube into the abdominal cavity, and close small abdominal incision. In the following intra-abodominal esophagogastrostomy, we can keep wide surgical view without the limitation due to the large remnant stomach and perform intra-abdominal anastomosis safely. We use over-lap method with liner staplers to perform the end to side anastomosis. After the anastomosis, we remake the angle of His to prevent gastroesophageal reflux.
Results and Conclusion: The intra-abdominal esophagogastrostomy using narrow gastric tube contribute to the wide surgical view under laparoscopy leading to the safety. Although our experience was limited, we found no complication, such as reflux esophagitis after operation, suggesting that small remnant stomach or end to side anastomosis contribute to prevent such complications.
Session: Poster
Program Number: P319

{kind=link}