Victor Avalos, MD, R Rumbaut, MD, H Guajardo, MD, Augusto Palomo, md, Z DEL Real, Guillermo PERalta. Hospital San Jose Tecnologico de Monterrey.
Introduction
Obese patients lose more weight with bariatric surgery than with medical weight-loss treatment. The laparoscopic Roux-en-Y gastric bypass (RYGB) procedure results in more short-term weight loss than laparoscopic adjustable gastric banding, but the latter has fewer postoperative complications and a lower mortality rate.
Prosthetic devices have been used in bariatric operations to control the outlet of the gastric pouch and thus maintain weight loss as well as marked gastrostomy site to decompressed distal gastric pouch with a gastrostomy. Marked gastrostomy site provides easy access to study distal bypassed stomach radiologically and/or endoscopically, as needed, access for enteral feeding in the rare case of excessive weight loss. A complication of these prostheses is erosion or migration into the gastric lumen.
Case report
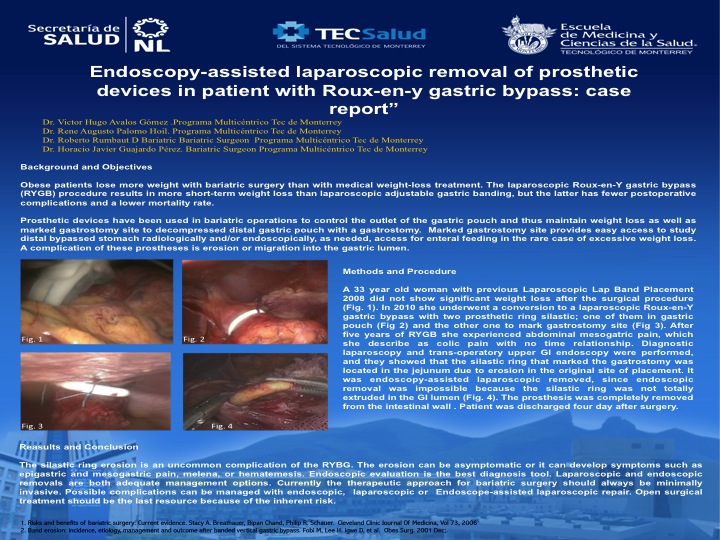
A 33 year old woman with previous Laparoscopic Lap Band Placement 2008 fig1 did not show significant weight loss after the surgical procedure. In 2010 she underwent a conversion to a laparoscopic Roux-en-Y gastric bypass with two prosthetic ring silastic; one of them in gastric pouch fig2 and the other one to mark gastrostomy site fig3. After five years of RYGB she experienced abdominal mesogatric pain, which she describe as colic pain with no time relationship. Diagnostic laparoscopy fig4 and trans-operatory upper GI endoscopy fig5 were performed, and they showed that the silastic ring that marked the gastrostomy was located in the jejunum due to erosion in the original site of placement. It was endoscopy-assisted laparoscopic removed, since endoscopic removal was impossible because the silastic ring was not totally extruded in the GI lumen.
Discussion
The silastic ring erosion is an uncommon complication of the RYBG. The erosion can be asymptomatic or it can develop symptoms such as epigastric and mesogastric pain, melena, or hematemesis. Endoscopic evaluation is the best diagnosis tool. Laparoscopic and endoscopic removals are both adequate management options.
Conclusion
Currently the therapeutic approach for bariatric surgery should always be minimally invasive. Possible complications can be managed with endoscopic, laparoscopic or Endoscope-assisted laparoscopic repair. Open surgical treatment should be the last resource because of the inherent risk.
fig 1 Fig2
Fig2 
Fig 3 Fig 4
Fig 4
Fig 5 
View Poster