I. Emre Gorgun, MD, Feza H Remzi, MD
Department of Colorectal Surgery, Digestive Disease Institute, Cleveland Clinic, Ohio
Introduction
Endoscopic submucosal dissection (ESD) has recently emerged as a novel technique to resect large colorectal lesions en bloc. Up to date no data exist regarding expansive ESD experiences from the United States. The aim of the present study was to report our case series on the first experiences and the learning challenges of ESD at a single colorectal surgery unit in the United States.
Patients and methods
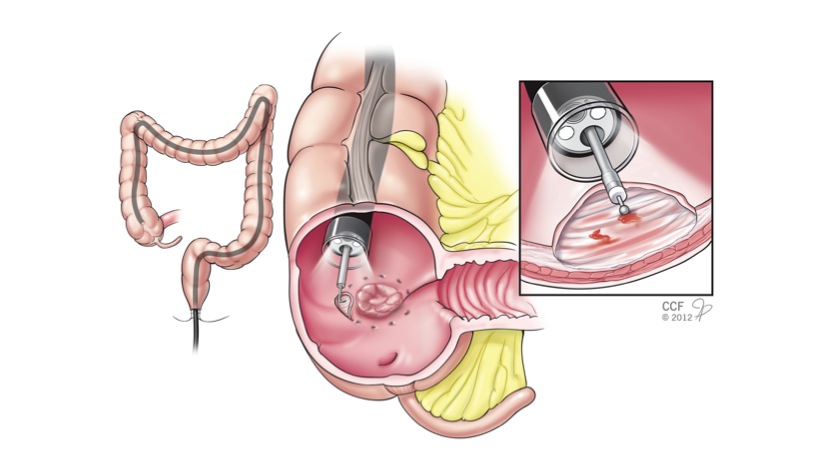
A total of 8 patients were referred for “Oncologic” colorectal resection (OCR) for large colorectal lesions. All studied patients were offered initial ESD procedure in the operating room with possible OCR if ESD could not be successfully completed. For the resection procedure conventional colonoscopes (PCF-H180AL, Olympus) were used and a transparent distal disposable cap was attached at the tip of the endoscope. Submucosal injection was performed using a mixture of saline, 2.5 % Hypromellose (Gonak, Akorn Incorporated, Somerset, NJ) and indigo carmine solution. The submucosal dissection was carried using dual knife, hook-knife and Coagrasper (Olympus Medical Systems, Tokyo, Japan) alternatively (Figure). Lesion characteristics, resection rates, procedure times, complications were recorded prospectively. Follow-up colonoscopy was performed at 3 months.
Results
There were eight patients (Five females). Median age of the patients was 66 (50-88); median ASA score was 4 (2-5); median BMI was 26 kg/m2 (18-41). Lesions were located in the cecum (50 %), Splenic flexure (25%) and the sigmoid colon (25%). ESD was possible in 6 lesions (75 %). Median operating time was 126 minutes (62-196). In 2 patients ESD could not be technically performed due to non-lifting of the lesion. For the remaining patients, there were no perforation or bleeding after ESD. Median length of hospital stay was 1 day (0-5). During follow up colonoscopy recurrence risk was 0 %.
Conclusions
The initial experiences in the United States confirm that ESD is feasible and effective with low complication rates and can avoid unnecessary oncologic segmental bowel resections. With growing ESD training courses and increasing experiences this approach will gradually expand and potentially more commonly used for large colonic lesions among American surgeons.
Session: Poster Presentation
Program Number: P588