Ahmed Alabbady, MD, Anthony Petrick, MD, FACS, Amrit A Rambhajan, MD, David M Parker, MD, FACS, Kathleen Johanson, DO, Vladin Obradovic, MD, Jon D Gabrielsen, MD, FACS, Anna R Ibele, MD
Geisinger Medical Center, Danville PA
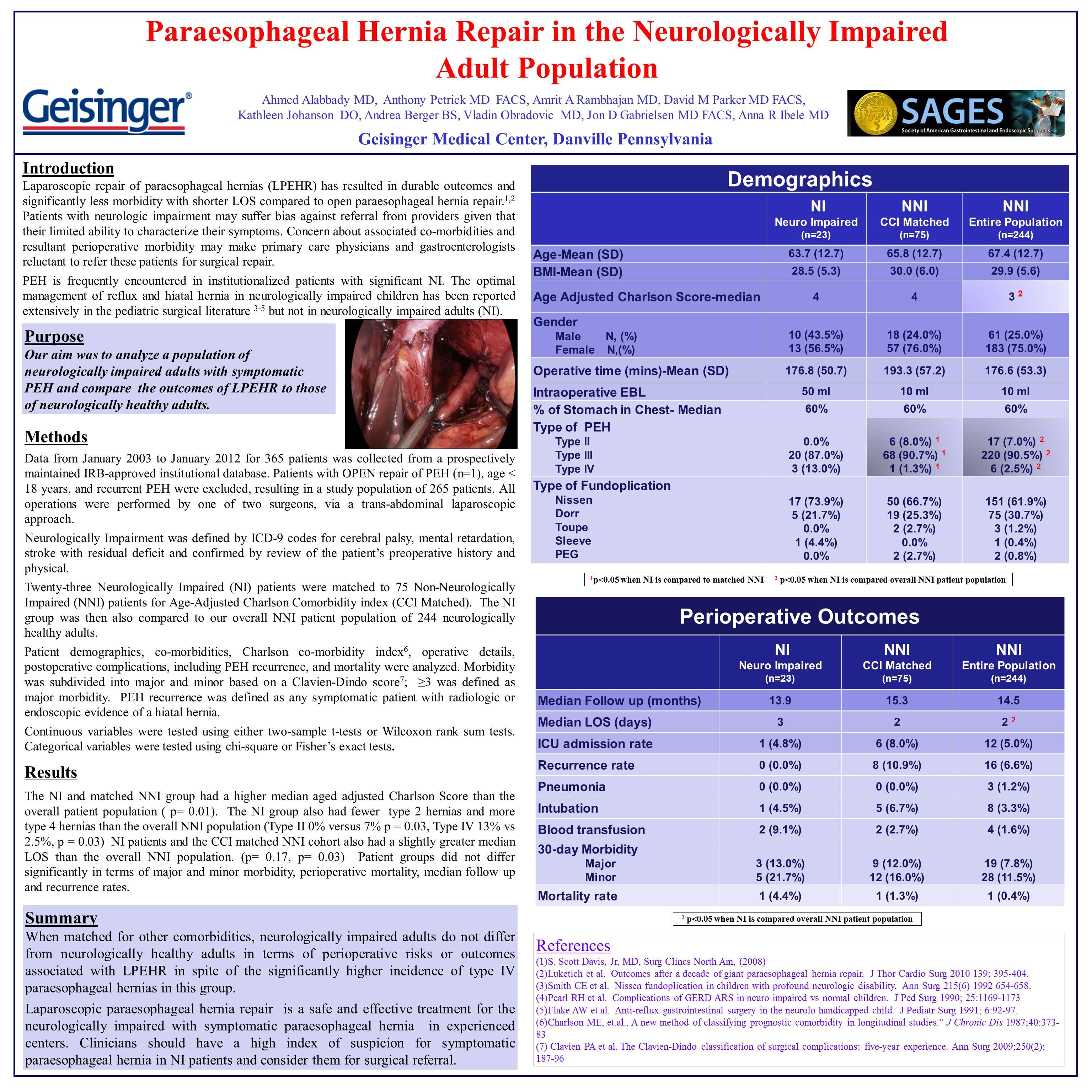
Background Paraesophageal hernia (PEH) is a difficult problem in neurologically impaired (NI) adults. Symptoms are difficult to assess and are often related through care givers. While outcomes of anti-reflux surgery in pediatric patients with neurologic impairment have been well studied, there are no large studies examining outcomes of paraesophageal hernia repair in the NI adult population. A better understanding of perioperative risks and specific outcomes would aid in counseling patients and their families. Our study goal was to analyze the perioperative outcomes and recurrence rate of our NI adult population undergoing laparoscopic PEH repair (LPEHR).
Methods We reviewed our prospectively maintained institutional database and identified twenty-nine adult patients with significant neurologic impairment (NI). This group was matched for age-adjusted Charlson comorbidity index to 99 patients with no history or clinical evidence of neurological disease at the time of the surgery (Non-Neurologically Impaired- NNI), and perioperative outcomes and recurrence rates were compared.
Results NI individuals were similar to their matched NNI controls in terms of mean age (64 years vs 67 years p = 0.37), BMI (29.2 vs 29.7 p = 0.75) and age adjusted Charlson score (5.2 vs 4.1 p = 0.25). The two groups did not differ statistically in terms of EBL, postoperative pneumonia, transfusion requirements, or need for prolonged intubation. ICU admission rates were similar (NI 3.7% versus NNI 8.2% p = 0.40).
Mean LOS was 3.7 days for the NI group and 3.5 days for the NNI group (p = 0.28). Thirty day morbidity rates were 4.8 % for the NI group and 2.3 % for the NNI group (p = 0.60) and mortality rates for the NI group were 3.4% and for the NNI group 1.0% (p = 0.35). Clinical and radiographic recurrence rates were similar for NI (3.1%) compared to NNI (7.1 % p = 0.51). Median follow up was significantly longer (24.5 months) for the NI group than for the NNI group (12 months; p = 0.04).
Conclusions PEH is not an uncommon problem in neurologically impaired adults, although symptoms are difficult to assess in this population. There is little published literature on the outcomes of PEHR in NI adult patients. Our study found that perioperative LPEHR outcomes in adult NI patients, including 30-day morbidity and mortality, were not significantly different than in NNI age-matched controls. While not statistically significant, recurrence rates were lower than age-matched NNI controls at over 2 year median follow-up. LPEHR was a safe and effective treatment for neurologically impaired adults with symptomatic PEH in our experienced center.
Session: Poster Presentation
Program Number: P233