Jeffrey D Hawel, MD, James C Ellsmere, FRCSC, FACS. Dalhousie University
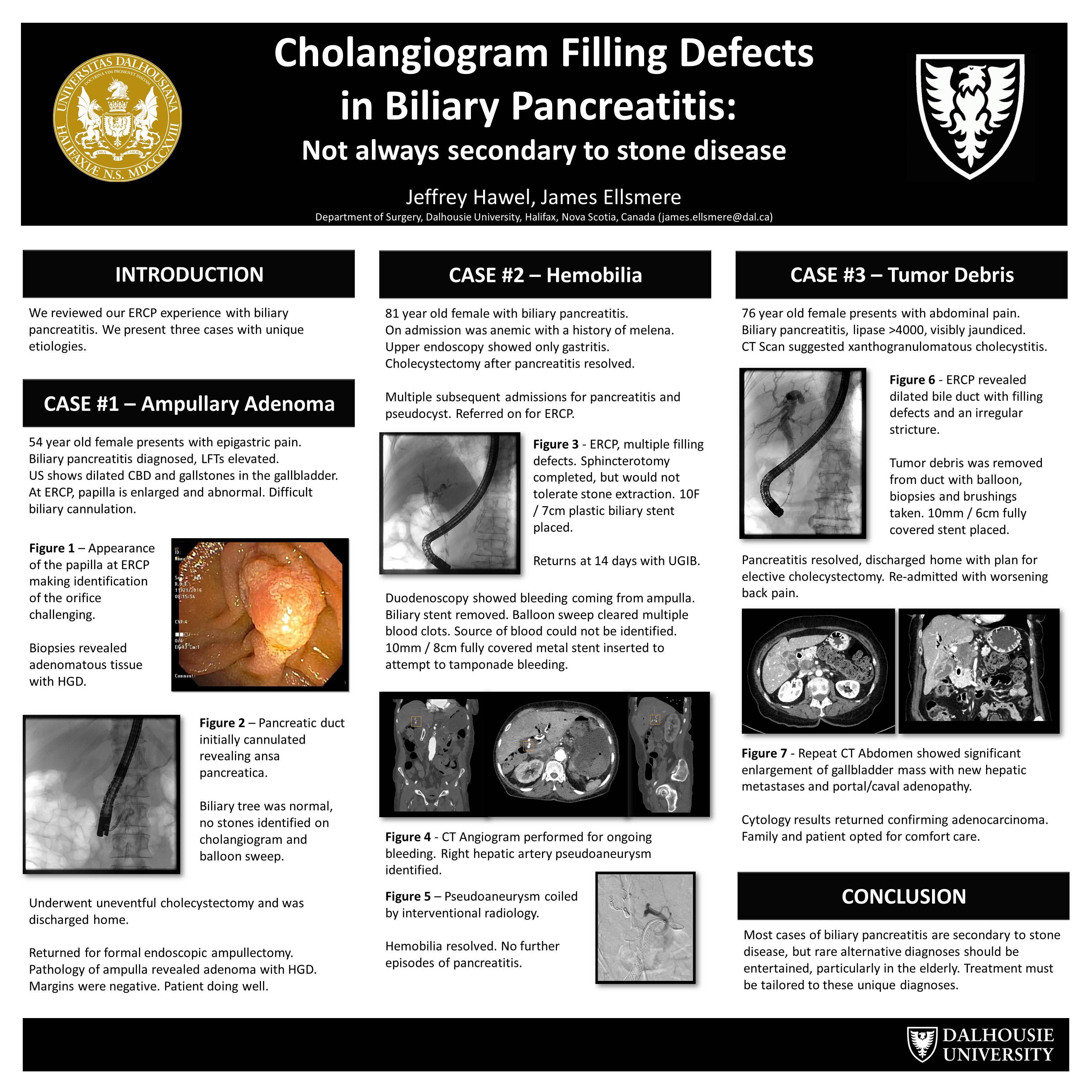
We reviewed our experience with biliary pancreatitis from July 2015 – September 2016. A total of 132 cases of biliary pancreatitis were managed on the therapeutic endoscopy service. All were confirmed to be secondary to stone or sludge in the biliary tree at the time of ERCP except for two cases. We present these two interesting cases of non-stone related biliary pancreatitis.
The first case was an 85-year old female admitted with biliary pancreatitis. MRCP showed a thickened gallbladder and cholelithiasis with intrahepatic duct dilation. Differential included Mirizzi syndrome versus locally invasive gallbladder cancer. The hepatobiliary service favored stone disease given the presentation with pancreatitis with planned open cholecystectomy. Pre-operative ERCP was requested. Multiple filling defects were confirmed in the distal bile duct on cholangiogram. Sphincterotomy and subsequent bile duct clearance revealed tumor debris. Brushings of common hepatic duct narrowing confirmed adenocarcinoma. The patient was effectively palliated with a biliary stent.
The second case was an 82-year old female with admission for severe biliary pancreatitis. She underwent uneventful cholecystectomy following resolution of her pancreatitis. Recurrent admissions were subsequently managed by the medicine service, due to comorbidities. Upon re-referral to therapeutic endoscopy, she underwent ERCP. Initial cholangiogram images showed multiple large filling defects within the common bile duct. Due to the length of procedure, bile duct clearance was deferred. She underwent a small sphincterotomy and stent placement. She had uneventful recovery and subsequent discharge. She was readmitted with melena two weeks later, and EGD and ERCP confirmed hemobilia with no evidence of bile duct stones. CT Angiography revealed a right hepatic artery aneurysm decompressing into the biliary tree, which was successfully coiled by interventional radiology. Final diagnosis was recurrent pancreatitis secondary to blood clot within the biliary tree.
The majority of filling defects on biliary imaging are stones or sludge, but as these cases illustrate other causes are possible. Additional causes described in the literature include foreign bodies like clips, and parasites. These alternative etiologies may require different management than the standard cholecystectomy and bile duct clearance.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 80902
Program Number: P338
Presentation Session: Poster (Non CME)
Presentation Type: Poster