Prashant Sinha, MD, MEng
New York University Langone Medical Center, Bellevue Hospital Center
Introduction: Morbidity in giant abdominal wall reconstruction may be significant in the early postoperative period from pain and wound complications, and from hernia recurrences long term. To improve outcomes, botulinum toxin A was applied to the oblique muscles to reduce postoperative incisional tension. The initial findings are reported from seven abdominal wall reconstructions in which botulinum toxin was used.
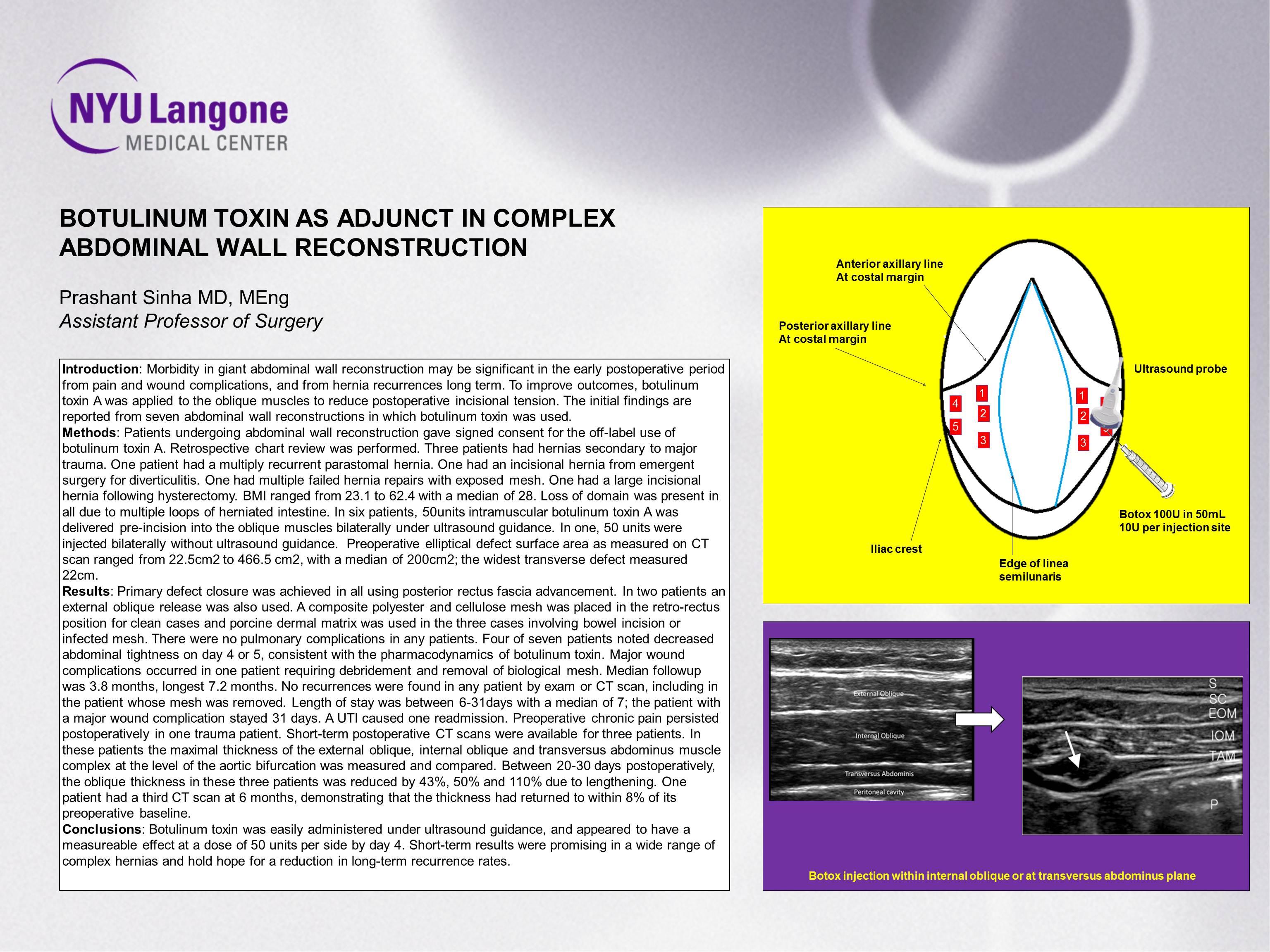
Methods: Patients undergoing abdominal wall reconstruction gave signed consent for the off-label use of botulinum toxin A. Retrospective chart review was performed. Three patients had hernias secondary to major trauma. One patient had a multiply recurrent parastomal hernia. One had an incisional hernia from emergent surgery for diverticulitis. One had multiple failed hernia repairs with exposed mesh. One had a large incisional hernia following hysterectomy. BMI ranged from 23.1 to 62.4 with a median of 28. Loss of domain was present in all due to multiple loops of herniated intestine. In six patients, 50units intramuscular botulinum toxin A was delivered pre-incision into the oblique muscles bilaterally under ultrasound guidance. In one, 50 units were injected bilaterally without ultrasound guidance. Preoperative elliptical defect surface area as measured on CT scan ranged from 22.5cm2 to 466.5 cm2, with a median of 200cm2; the widest transverse defect measured 22cm.
Results: Primary defect closure was achieved in all using posterior rectus fascia advancement. In two patients an external oblique release was also used. A composite polyester and cellulose mesh was placed in the retro-rectus position for clean cases and porcine dermal matrix was used in the three cases involving bowel incision or infected mesh. There were no pulmonary complications in any patients. Four of seven patients noted decreased abdominal tightness on day 4 or 5, consistent with the pharmacodynamics of botulinum toxin. Major wound complications occurred in one patient requiring debridement and removal of biological mesh. Median followup was 3.8 months, longest 7.2 months. No recurrences were found in any patient by exam or CT scan, including in the patient whose mesh was removed. Length of stay was between 6-31days with a median of 7; the patient with a major wound complication stayed 31 days. A UTI caused one readmission. Preoperative chronic pain persisted postoperatively in one trauma patient. Short-term postoperative CT scans were available for three patients. In these patients the maximal thickness of the external oblique, internal oblique and transversus abdominus muscle complex at the level of the aortic bifurcation was measured and compared. Between 20-30 days postoperatively, the oblique thickness in these three patients was reduced by 43%, 50% and 110% due to lengthening. One patient had a third CT scan at 6 months, demonstrating that the thickness had returned to within 8% of its preoperative baseline.
Conclusions: Botulinum toxin was easily administered under ultrasound guidance, and appeared to have a measureable effect at a dose of 50 units per side by day 4. Short-term results were promising in a wide range of complex hernias and hold hope for a reduction in long-term recurrence rates.
Session: Poster Presentation
Program Number: P286