Salinas José, MD, Rodrigo Fernandez, MD, César Muñoz, MD, Julio Cerda, MS, Luis Ibáñez, MD, Fernando Crovari, MD, Gustavo Pérez, MD, Ricardo Funke, MD, Camilo Boza, MD. Department of Digestive Surgery. Hospital Clínico P. Universidad Católica de Chile
INTRODUCTION
Patients with BMI 30-35 kg/m2 and comorbidities that are refractory to intensive medical therapy are excluded from classic NIH Bariatric Surgery guidelines. The aim of this study is to compare Laparoscopic Sleeve Gastrectomy (LSG) to Laparoscopic Roux-en-Y gastric bypass (LRYGB) in patients with a preoperative BMI between 30-35 kg/m2 in terms of complication and weight loss
METHODS AND PROCEDURES
All cases were approved by a multidisciplinary team. All patients had at least one obesity-related comorbidity and several documented failed medical weight-loss treatment attempts. A review of our prospective electronic database between December 2002 and December 2010. Data is expresed as mean ± standard deviation or median (interquantile range) when appropiate.
RESULTS
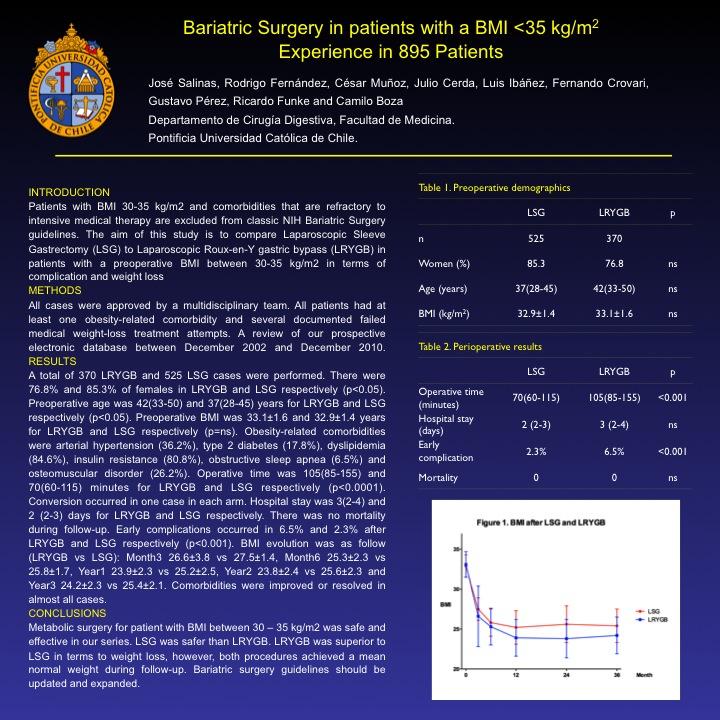
A total of 370 LRYGB and 525 LSG cases were performed. There were 76.8% and 85.3% of females in LRYGB and LSG respectively (p<0.05). Preoperative age was 42(33-50) and 37(28-45) years for LRYGB and LSG respectively (p<0.05). Preoperative BMI was 33.1±1.6 and 32.9±1.4 years for LRYGB and LSG respectively (p=ns). Obesity-related comorbidities were arterial hypertension (36.2%), type 2 diabetes (17.8%), dyslipidemia (84.6%), insulin resistance (80.8%), obstructive sleep apnea (6.5%) and osteomuscular disorder (26.2%). Operative time was 105(85-155) and 70(60-115) minutes for LRYGB and LSG respectively (p<0.0001). Conversion occurred in one case in each arm. Hospital stay was 3(2-4) and 2 (2-3) days for LRYGB and LSG respectively. There was no mortality during follow-up. Early complications occurred in 6.5% and 2.3% after LRYGB and LSG respectively (p<0.001). BMI evolution was as follow (LRYGB vs LSG): Month3 26.6±3.8 vs 27.5±1.4, Month6 25.3±2.3 vs 25.8±1.7, Year1 23.9±2.3 vs 25.2±2.5, Year2 23.8±2.4 vs 25.6±2.3 and Year3 24.2±2.3 vs 25.4±2.1. Comorbidities were improved or resolved in almost all cases.
CONCLUSION
Metabolic surgery for patients with a BMI between 30 – 35 kg/m2 was safe and effective in our series. LSG was safer than LRYGB. LRYGB was superior to LSG in terms to weight loss, however, both procedures achieved a mean normal weight during follow-up. Bariatric surgery guidelines should be updated and expanded.
Session Number: Poster – Poster Presentations
Program Number: P494
View Poster