Introduction: Gastrostomy tube dislodgment shortly after placement may lead to a gastric perforation if a gastrocutaneous fistula tract did not have time to form. The current standard approach to this problem is immediate laparotomy and creation of a new gastrostomy. We report a novel, incision-free approach to this problem that involves grasping the gastric perforation with an optical bronchoscope through the previous abdominal wall incision.
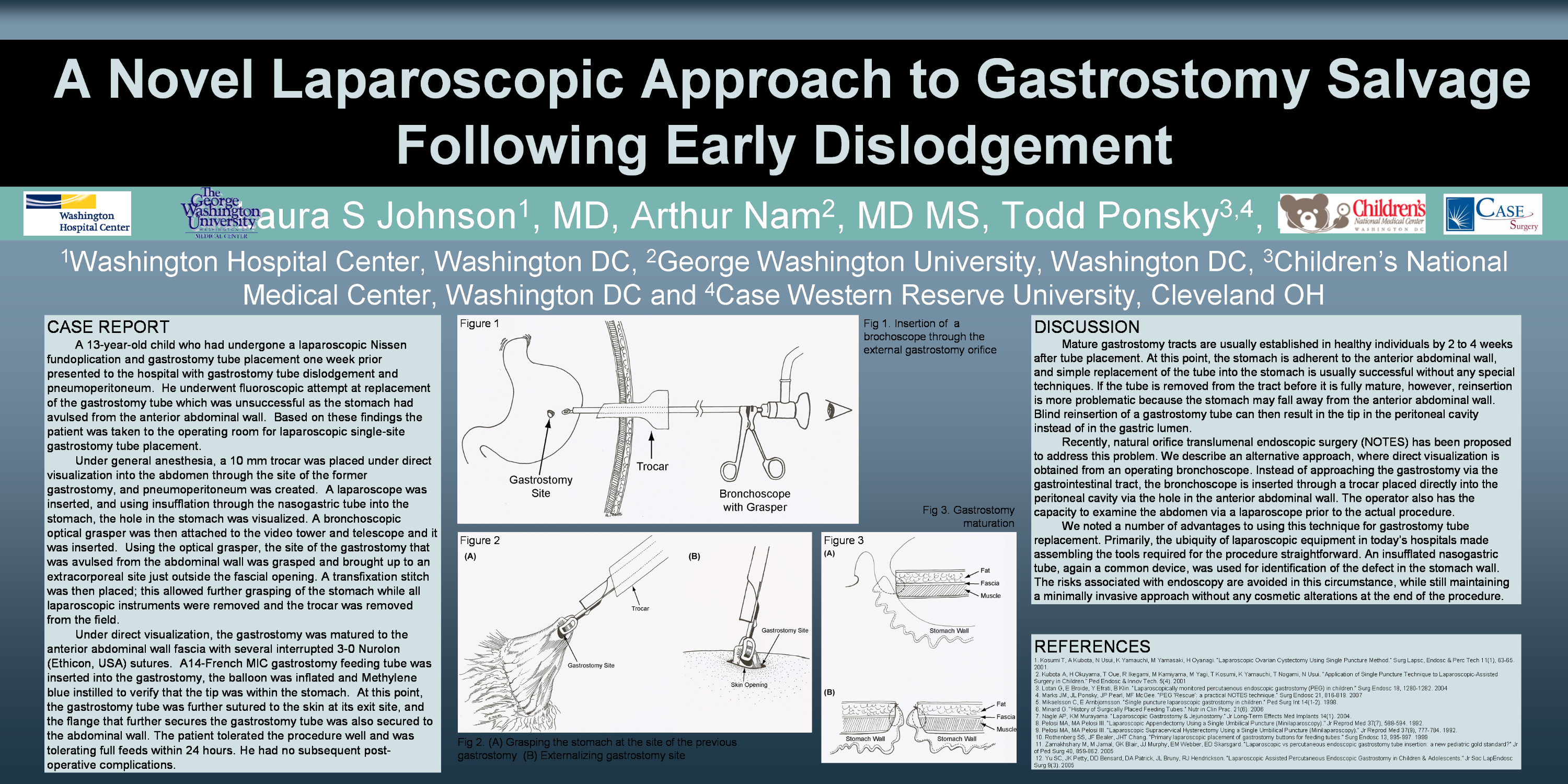
Case Report and Description of Procedure: A 13-year-old child who had undergone a laparoscopic Nissen and gastrostomy tube placement one week prior presented to the hospital with gastrostomy tube dislodgement and pneumoperitoneum. He underwent fluoroscopic attempt at replacement of the gastrostomy tube which was unsuccessful as the stomach had avulsed from the anterior abdominal wall. Based on these findings the patient was taken to the operating room for laparoscopic single-site gastrostomy tube placement.
Through the site of the former gastrostomy, a 5 mm trocar was placed under direct visualization into the abdomen and a pneumoperitoneum was created. A laparoscope was inserted and the hole in the stomach was visualized. A bronchoscopic optical grasper was then inserted. Using the optical grasper, the site of the gastrotomy that was avulsed from the abdominal wall was grasped and brought up to an extracorporeal site just outside the fascial opening. A transfixation stitch was placed at that point; this allowed further grasping of the stomach while all laparoscopic instruments were removed and the trocar was removed from the field. Under direct visualization, the gastrotomy was matured to the anterior abdominal wall fascia with several interrupted 3-0 Nurolon (Ethicon, USA) sutures. Under direct visualization, a 14-French gastrostomy feeding tube was inserted into the gastrotomy. The balloon was inflated. Methylene blue was then instilled into the gastrostomy tube, and the methylene blue, following aspiration of the NG tube, verified that the tip was within the stomach. The patient tolerated the procedure well and was tolerating full feeds after 2days. He had no subsequent post-operative complications.
Conclusion: This single site, optical grasper, approach to gastrostomy salvage is minimally invasive and an easy approach to early gastrostomy dislodgement
Session: Poster
Program Number: P142

{kind=link}