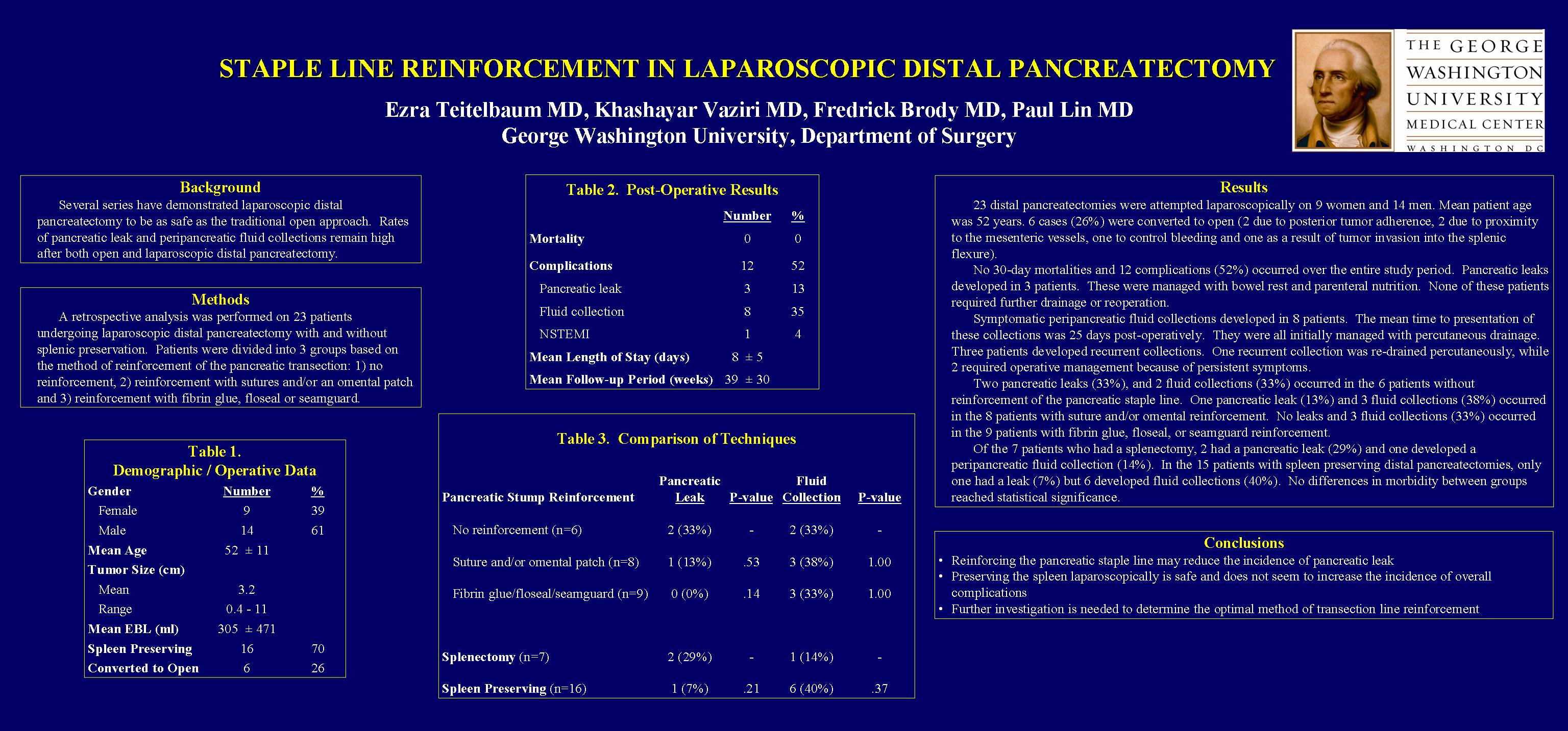
Objectives: Several series document that laparoscopic distal pancreatectomy is as safe as the traditional open approach. However, pancreatic leaks and peri-pancreatic fluid collections remain common morbidities. This report analyzes three methods of staple line reinforcement following laparoscopic distal pancreatectomy, with and without splenic preservation, with regards to post-operative pancreatic fistulas and peri-pancreatic fluid collections.
Methods: A retrospective analysis was performed on 23 patients undergoing laparoscopic distal pancreatectomy with and without splenic preservation from November 2003 to August 2009. Clinical, demographic, operative and postoperative data were recorded. Patients were divided into three groups based upon the type of reinforcement used on the transection line. These groups included (1) no additional reinforcement, (2) suture or omental reinforcement, or (3) the use of fibrin glue, flowseal or seamguard. A chi-squared test was used to statistically assess differences in morbidity between groups.
Results: 23 laparoscopic distal pancreatectomies were performed. The mean patient age was 52 ±11 years, and 14 patients were female (61%). Mean follow-up time was 39 ±30 weeks. Conversion to open occurred in 6 cases (26%), and the spleen was preserved in 16 cases (70%). Median blood loss was 150ml, and median length of stay was 7 ±4 days. The mean size of pancreatic lesions was 3.4 ±2.5cm. Pancreatic fistulas occurred in 3 cases (13%), while peri-pancreatic fluid collections developed in 8 cases (34%). There was one mortality (4%) that occurred three months postoperatively from metastatic pancreatic adenocarcinoma. No additional reinforcement was used in 6 patients (26%). Suture reinforcement and/or an omental patch were used in 8 patients (35%). Reinforcement materials such as fibrin glue, floseal or seamguard were used in 9 cases (39%). Two pancreatic fistulas (33%), and 2 fluid collections (33%) occurred in the group without reinforcement. One pancreatic fistula (13%) and 3 fluid collections (38%) occurred in the group with suture/omental reinforcement. No fistulas and 3 fluid collections (33%) occurred in the group with fibrin glue, floseal, or seamguard reinforcement. Although a trend of decreased pancreatic fistulae with reinforcement was observed, this did not reach statistical significance. Splenic preservation did not affect morbidity.
Conclusions: This series of laparoscopic distal pancreatectomies is comparable with previously reported results in terms of overall morbidity, pancreatic fistula and peri-pancreatic fluid collection rates. Reinforcement of the pancreatic transection line may reduce the incidence of pancreatic fistula. Splenic preservation did not seem to affect the incidence of morbidity. Further investigation is needed to determine the optimal method of pancreatic transection line reinforcement.
Session: Poster
Program Number: P429

{kind=link}