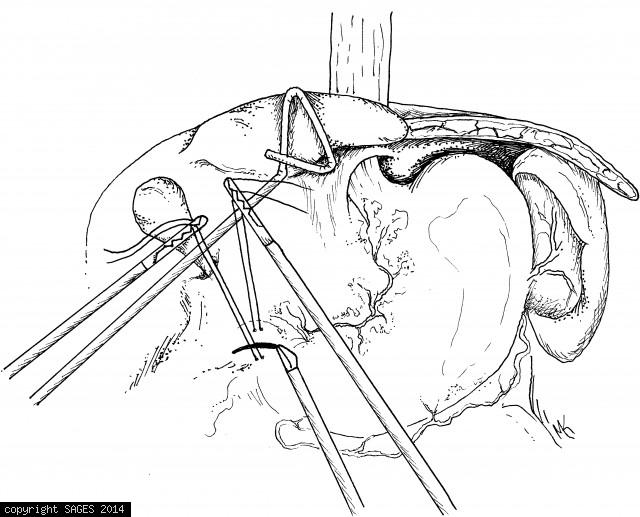
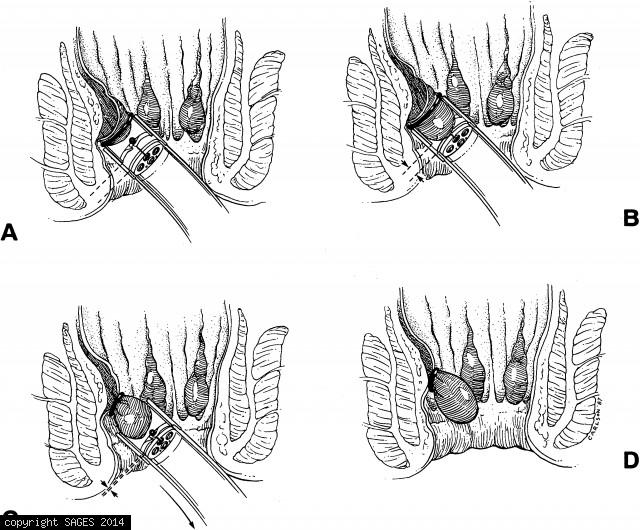
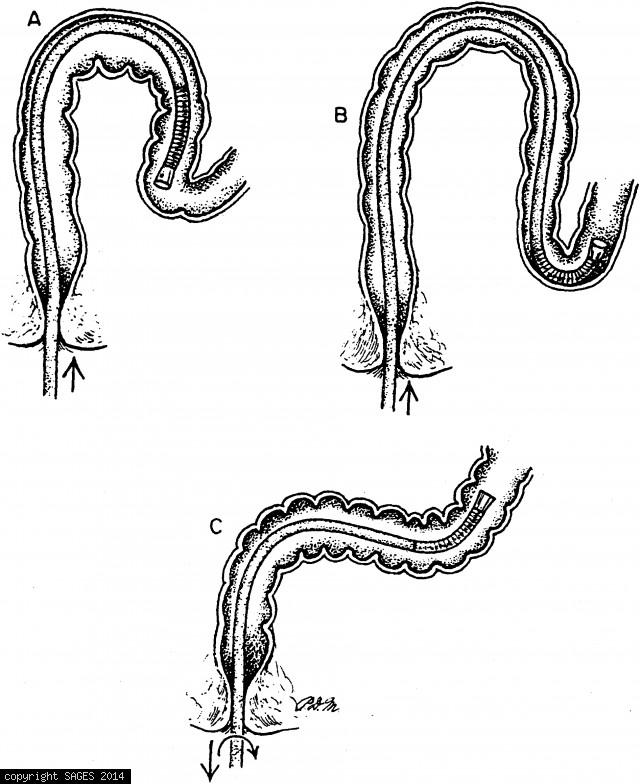
Completed abdominal myotomy
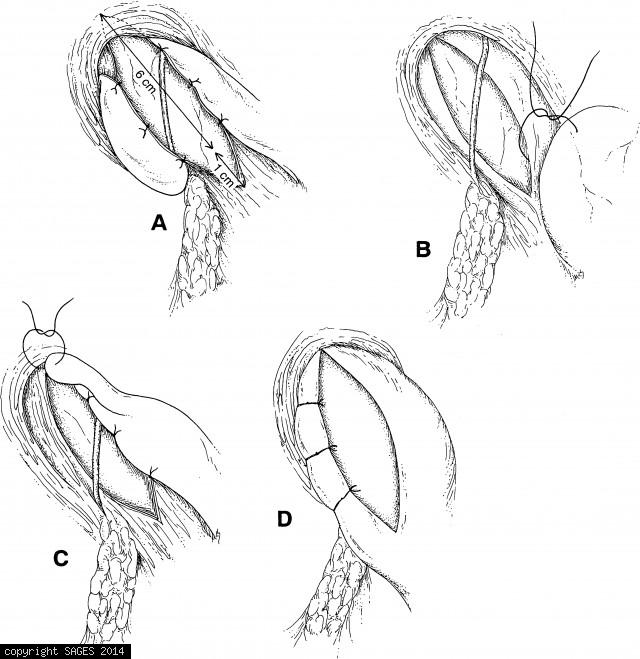
A. Completed abdominal myotomy with Toupet posterior fundoplication. B–D. Completed abdominal myotomy with Dor anterior fundoplication. (Reprinted with permission from Hunter et al, Laparoscopic Heller myotomy and fundoplication for achalasia. Ann Surg 1
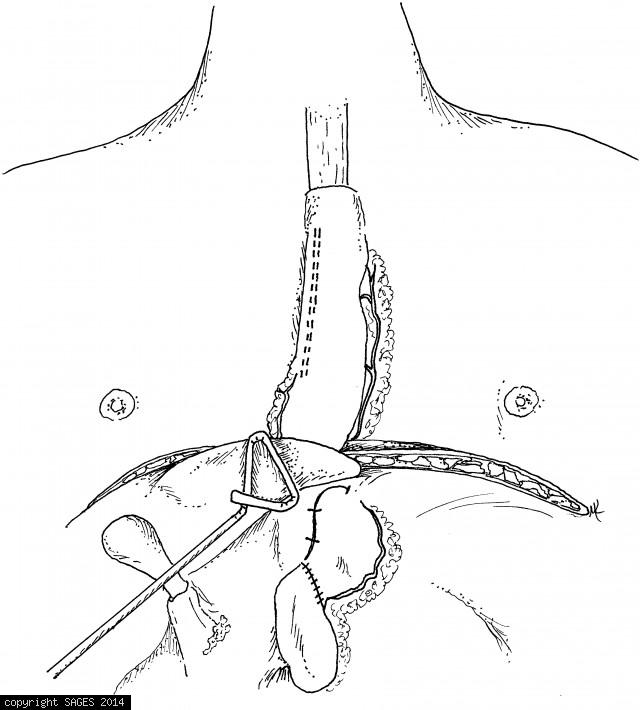
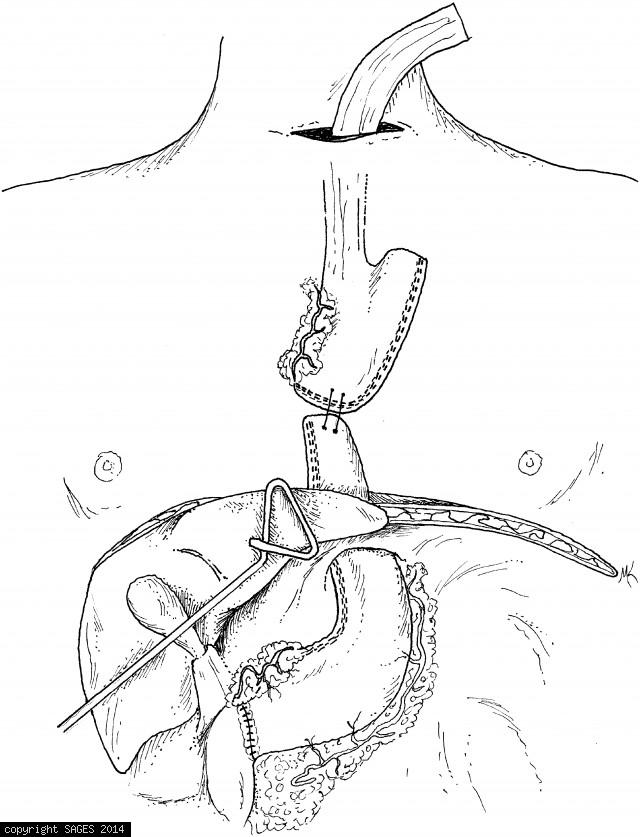
Attaching esophageal & gastric tube

Attaching the esophageal and gastric tube prior to mobilization.


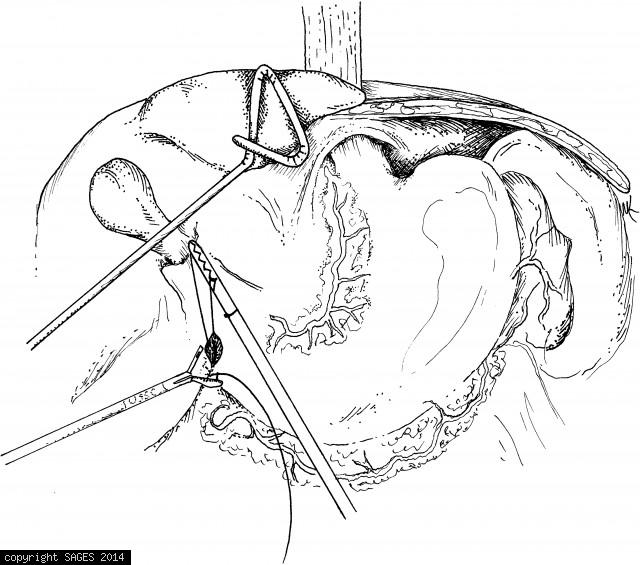
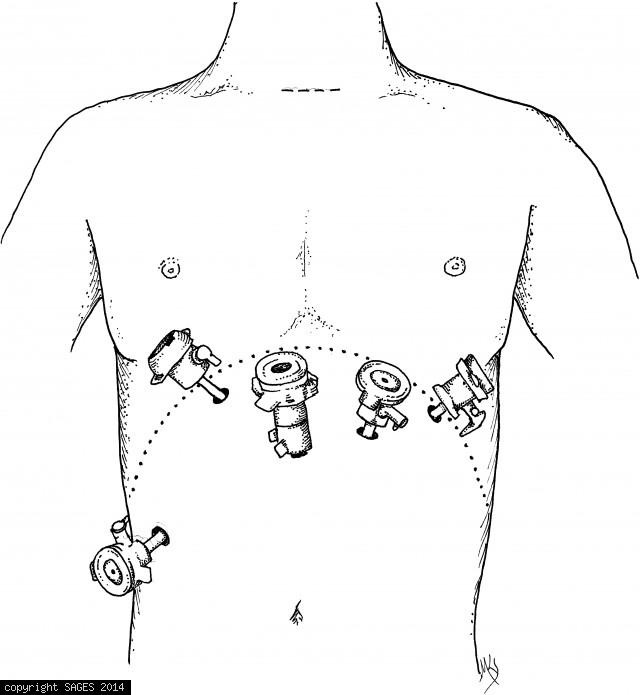
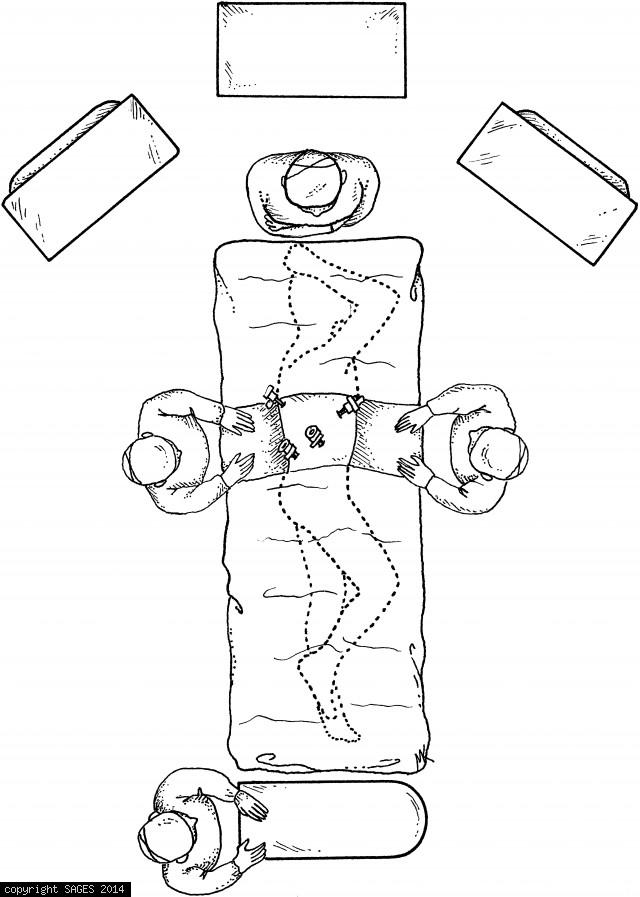
Setup gastric mobilization & tubularizarization

Room setup for gastric mobilization and tubularization.

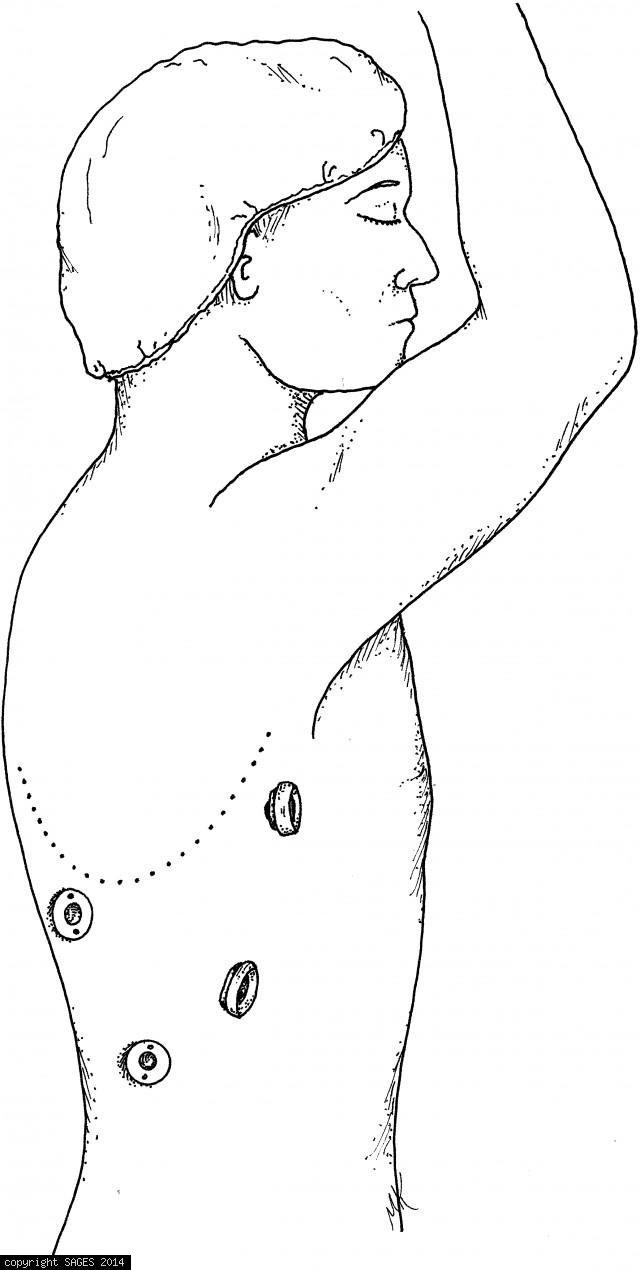
Room setup thoracoscopic esophageal mobilization
Room setup for thoracoscopic esophageal mobilization.
Direct endoscopic ligation of internal hemorrhoids
Direct endoscopic ligation of internal hemorrhoids. A. The endoscopist positions the ligator in contact with the hemorrhoid about 1 cm above he dentate line. B. Endoscopic suction draws the hemorrhoid into the banding cylinder. C. The elastic O-ring is ej
System of T tumor-staging of rectal cancers

System of T tumor-staging of rectal cancers based upon endoscopic ultrasound appearance.
Formation of loops in the colon
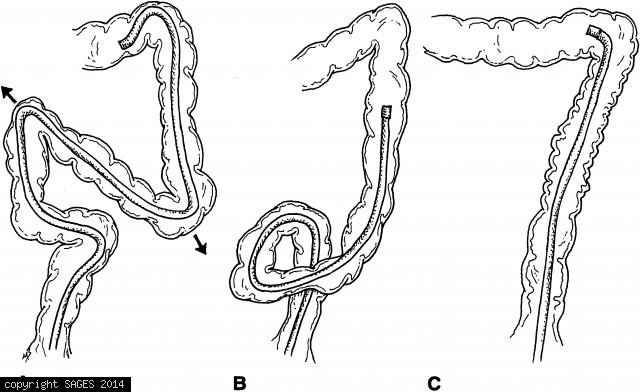
A. Formation of loops in the colon can cause patient discomfort, difficulty in advancing the scope, and may increase the risk of perforation. B. Here an alpha loop has been formed in the sigmoid colon, facilitating passage into the descending colon. Clock
Patient position and room setup
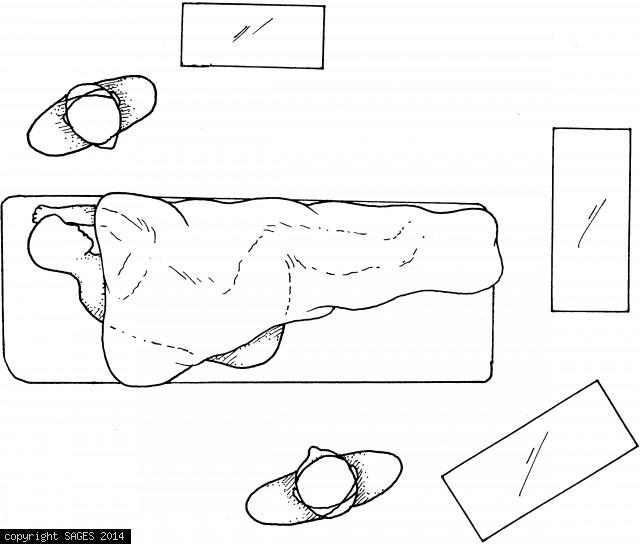
Patient position and room setup. A video monitor is placed in the direct line of sight of the endoscopist (at the back of the patient) and the assistant (who stands in front of the patient). Monitoring equipment for EKG, blood pressure, and oxygen saturat
Intubation by dither-torquing

Intubation by dither-torquing. A. The shaft is torqued counterclockwise while advancing the shaft 10 to 15cm. B. The shaft is torqued clockwise while withdrawing the shaft 10 to 15 cm. Repetition of this cycle encourages the sigmoid to accordionize onto
Intubation by looping
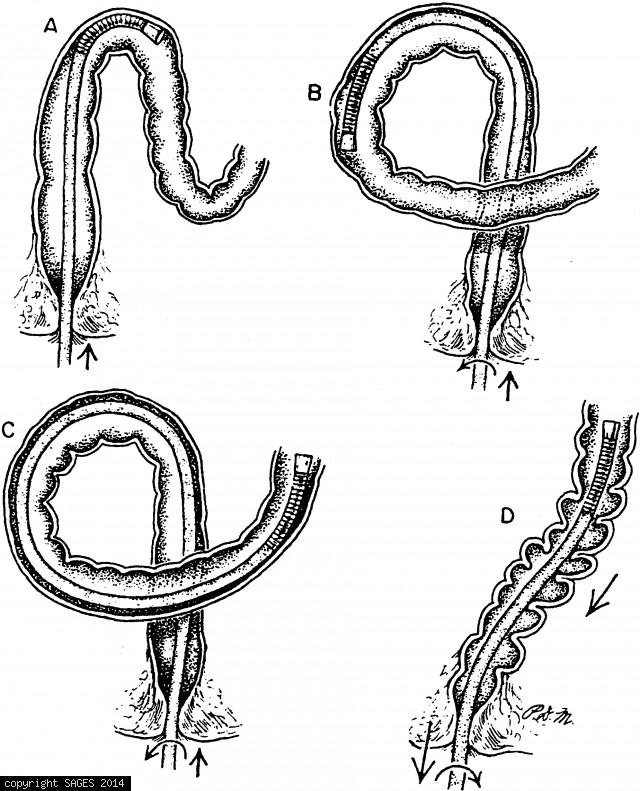
Intubation by looping. A. The sigmoidoscope is advanced to the distal sigmoid. B. Counterclockwise torquing during further advancement loops the proximal sigmoid in front of the distal sigmoid. C. The looped sigmoid flattens the angle at the distal-descen
Intubation by elongation
Intubation by elongation. A. The sigmoidoscope is advanced to the proximal sigmoid. B. Severe tip deflection prevents further advancement resulting in sigmoid elongation. C. Clockwise torquing and shaft withdrawal accordionizes the sigmoid.

Bile duct cannulation
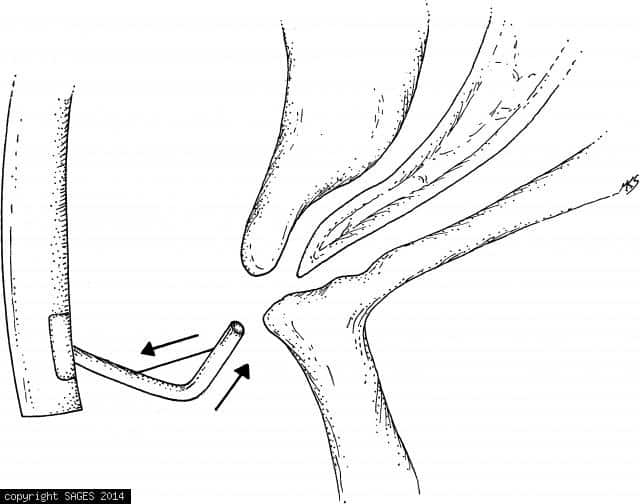
Sometimes bile duct cannulation requires orientation of the cannula in a cephalad direction. This can be accomplished by using a sphincterotome. Tightening the cutting wire bows the cannula upward and produces a more cephalad orientation for the tip of th
Lifting the cannula
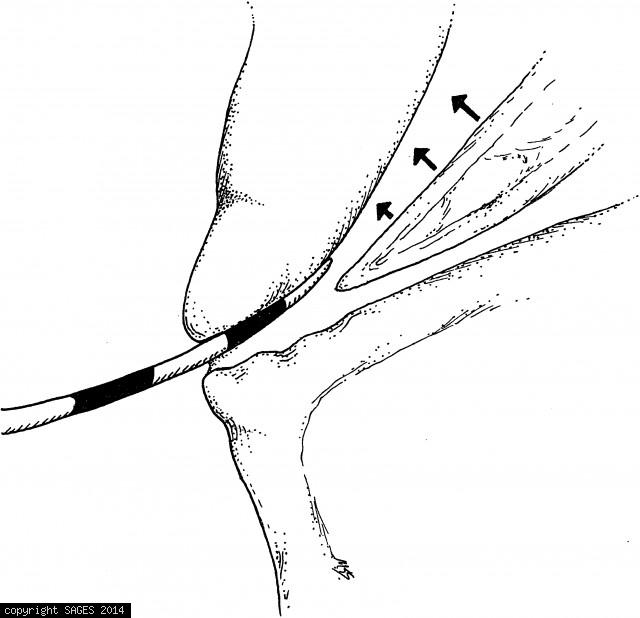
Lifting the cannula to insert it along the “roof ” of the papilla increases the likelihood of entry into the bile duct.
The “tucked under” position
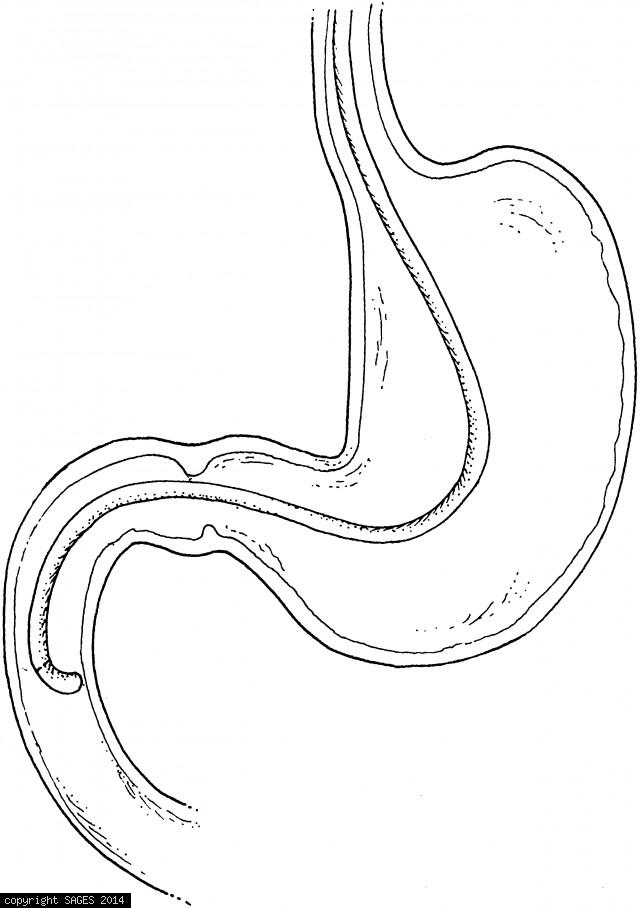
The “tucked under” position is usually obtained by advancing the endoscope slightly and deflecting the tip upward.