View of Pylorus

View of pylorus. Bubbles indicating bile provide a clue to the location of the distal stomach when orientation of the side-viewing endoscope is difficult.
PEG tube

The PEG tube is pulled back into the stomach. Endoscopic verification of placement is essential.
Transillumination and finger depression

A. Transillumination and finger depression of the abdominal wall confirm juxtaposition of the inflated stomach and the anterior abdominal wall. B. The site selected will generally be approximately halfway between costal margin and umbilicus.
Patient Positioning
With the patient in the left lateral decubitus position, the endoscopist facing the patient, and the scope relaxed as described in the text, entry into the stomach will generally give a view oriented with the lesser curvature at 12 o’clock, the greater cu
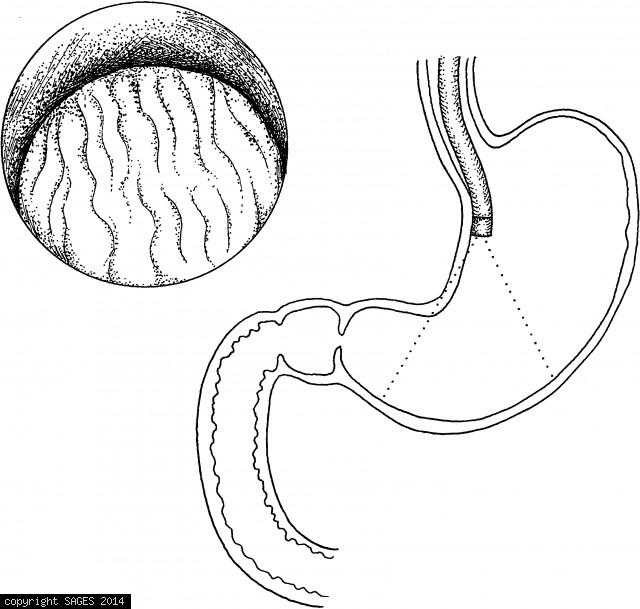
Upper Gastrointestinal Endoscopy
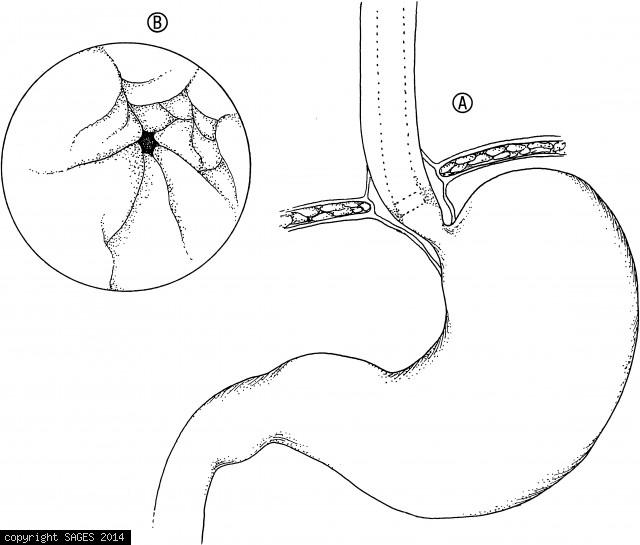
A. The endoscope is advanced down the relatively straight esophagus until the lower esophageal sphincter is identified. B. The lower esophageal sphincter often coincides with the transition from squamous epithelium (white) of the esophagus to mucosa (pink
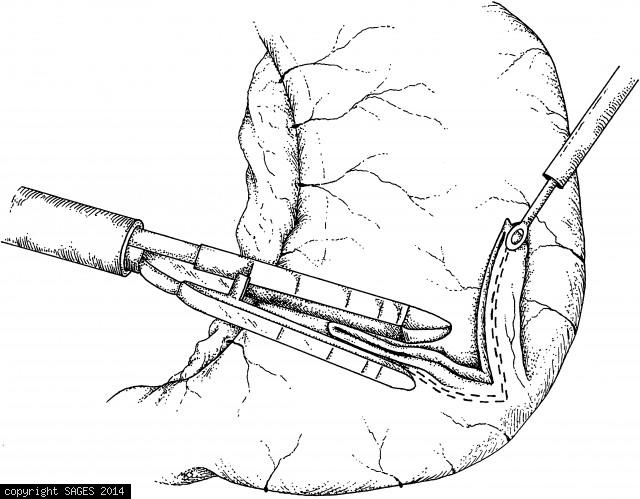
Selecting and Affixing loop of jejunum
A loop of jejunum has been selected and affixed to the greater curvature of the stomach, above the gastroepiploic vessels, with two stay sutures. Two enterotomies have been made and the stapling device inserted.
Trocar Placement

Trocar placement for gastrojejunostomy is slightly different, in that trocar 2 is placed lower, to allow adequate working distance from the stomach. If you plan to do both procedures, use this trocar arrangement (rather than that in Fig. 36.1).
Retracting the stomach cephalad
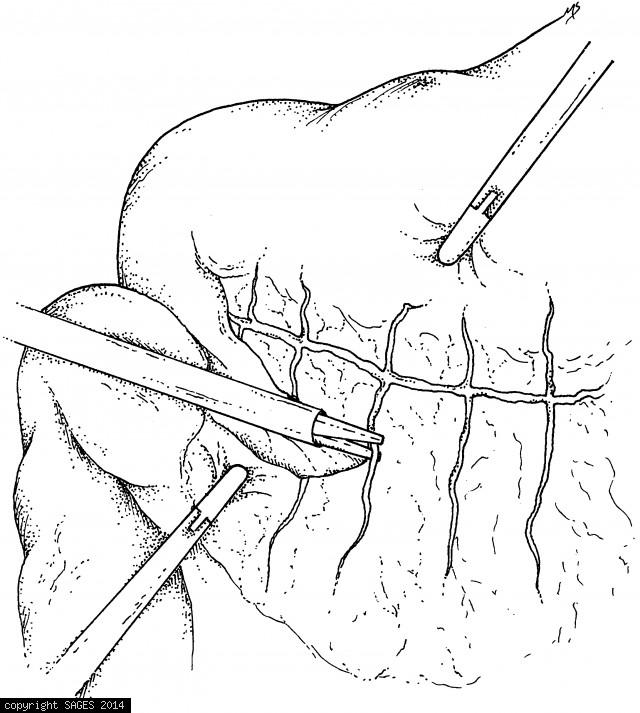
The stomach is retracted cephalad as the transverse colon is retracted caudad while the omentum is divided with the harmonic scalpel.
Gastric Balloon catheter to facilitate pouch
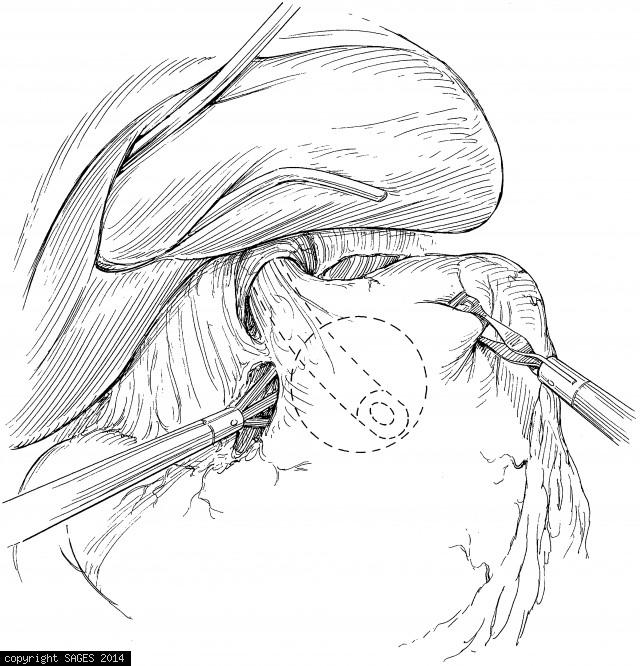
The stomach is exposed and mobilized. A gastric balloon catheter may be used to define the pouch and facilitate pouch creation. (Soper NJ, Swanstrom LL, Eubanks WS, eds. Mastery of Endoscopic and Laparoscopic Surgery. 2d ed. Philadelphia: Lippincott Willi
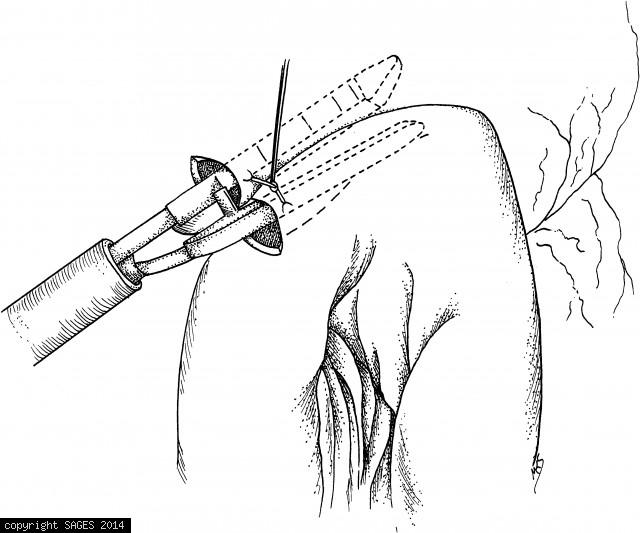
Insertion of the Innerdyne gastric cannula

Insertion of the Innerdyne gastric cannula into inflated stomach. Thereafter, the radially expandable polymer sheath is stretched by an 11.0-mm port for intragastric insertion of the operating laparoscope.
Construction of mucosa-lined tube
Construction of mucosa-lined tube (Janeway-style gastrostomy). A fold of stomach is elevated and the endoscopic stapler applied. Approximately 1 cm of stomach must be included in the staple line to assure an adequate lumen. The tube is grasped and elevate
Myotomy carried distally by hook Electrocautery
The myotomy being carried distally, using hook electrocautery. Care must be taken to elevate the muscle fibers away from the mucosa before the electrocautery is applied. The myotomy extends about 5 to 6 cm proximal to the gastroesophageal junction and abo
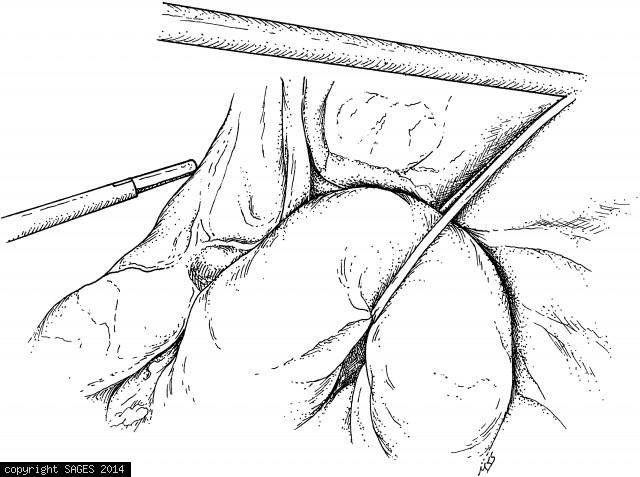
Mobilization of the fundus

Retract the stomach rightward and the spleen and omentum left and downward to complete mobilization of the fundus. These maneuvers open the lesser sac and facilitate division of the high short gastric vessels.
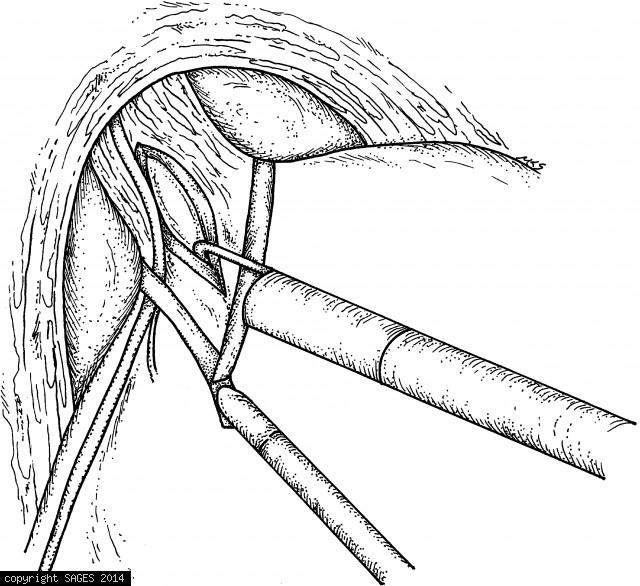
Dissection of the left crus

Dissection of the left crus. The left crus is dissected as completely as possible, and the attachments of the fundus of the stomach to the diaphragm are taken down.