Abdelrahman A Nimeri, MD, FACS, FASMBS, Ahmed O Maasher, MD, Maha Ibrahim, MD, Mohammed Al Haddad, MD. Sheikh Khalifa Medical City
Introduction:
Laparoscopic sleeve gastrectomy (LSG) is an acceptable primary operation for morbid obesity. Leak after LSG is one of the most serious complications. However, all leaks after LSG are not the same and they differ based on the timing of presentation, and presence of peritonitis or distal stricture. Different management strategies have been described including endoscopic stents, or surgical correction. However, no clear algorithm has been described for management.
Objectives:
Describe our experience in managing leaks after LSG and describe our management algorithm.
Methods:
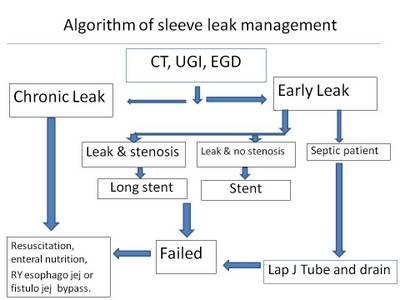
We reviewed our prospectively maintained database for all LSG performed and all leaks after LSG treated at BMI Abu Dhabi from September 2009 to 2014. In addition, we reviewed the literature for management strategies for patients with leaks after LSG including endoscopic and operative strategies. Leaks are considered early in the first 6 weeks and chronic after 12 weeks of LSG. The corner stone in our managment is enteral feeding through a nasojejunal feeding or jejunostomy tube. In addition, the timing of the leak, the presence of a distal stenosis/stricture and the presence of peritonitis dictate our management approach. Our initial evaluation includes gastrograffin studies, CT of the Abdomen and upper endoscopy. All chronic leaks and early leaks with distal stenosis not amenable to endoscopic stening were treated with optimization followed by laparoscopic Roux en Y esophago jejunostomy. Early leaks with or without peritonitis were treated with laparoscopy drainage and jejunostomy feeding and endoscopic stents respectively.
Results:
Between September 2009 and 2014 we performed 236 LSG procedures without a leak. During the same time period we treated 15 patients with leaks after LSG referred to our unit according to our management strategy described above. Three patients were treated with laparoscopic esophago jejunostomy without complications. Eight patients were treated with exploration and jejunostomy tube placement and the remaining patients were treated conservatively with or without stents. All patients were started on enteral and sent home once their sepsis is controlled. Our success rate with endoscopic stents was 50% while our success rate after operative correction was 100%. Our mortality rate was zero.
Conclusion:
All leaks after LSG are not the same. The management strategy at BMI Abu Dhabi depends on enteral feeding, the timing of presentation, and presence of peritonits stiricture.