J Koury, MD, P Maxwell, MD, G Isenberg, MD, S Goldstein, MD. Thomas Jefferson University
Introduction: The reported acceptable incidence of anastomotic leak following a colon resection is reported to be approximately 3-6%. Some authors have noted a 1% leak rate for right colectomy occurring within 30 days of the procedure. While this is the traditional time period during which most leaks occur, clinically significant leaks can occur greater than 30 days post-resection which we refer to as a delayed leak. Although the concept of a delayed leak has been described, data regarding the presentation and timing remains limited. We retrospectively reviewed our database and present patient characteristics and presentation for 3 delayed leaks following right colectomy.
Methods: We retrospectively reviewed our database of three colorectal surgeons from February 2010 to March 2011. The incidence of a delayed leak occurring greater than 30 days from an ileocolic anastomosis, time of presentation of leak, and treatment were noted. Leaks were identified using standard radiological methods including but not limited to computed tomography (CT), gastrograffin enema, and plain abdominal films.
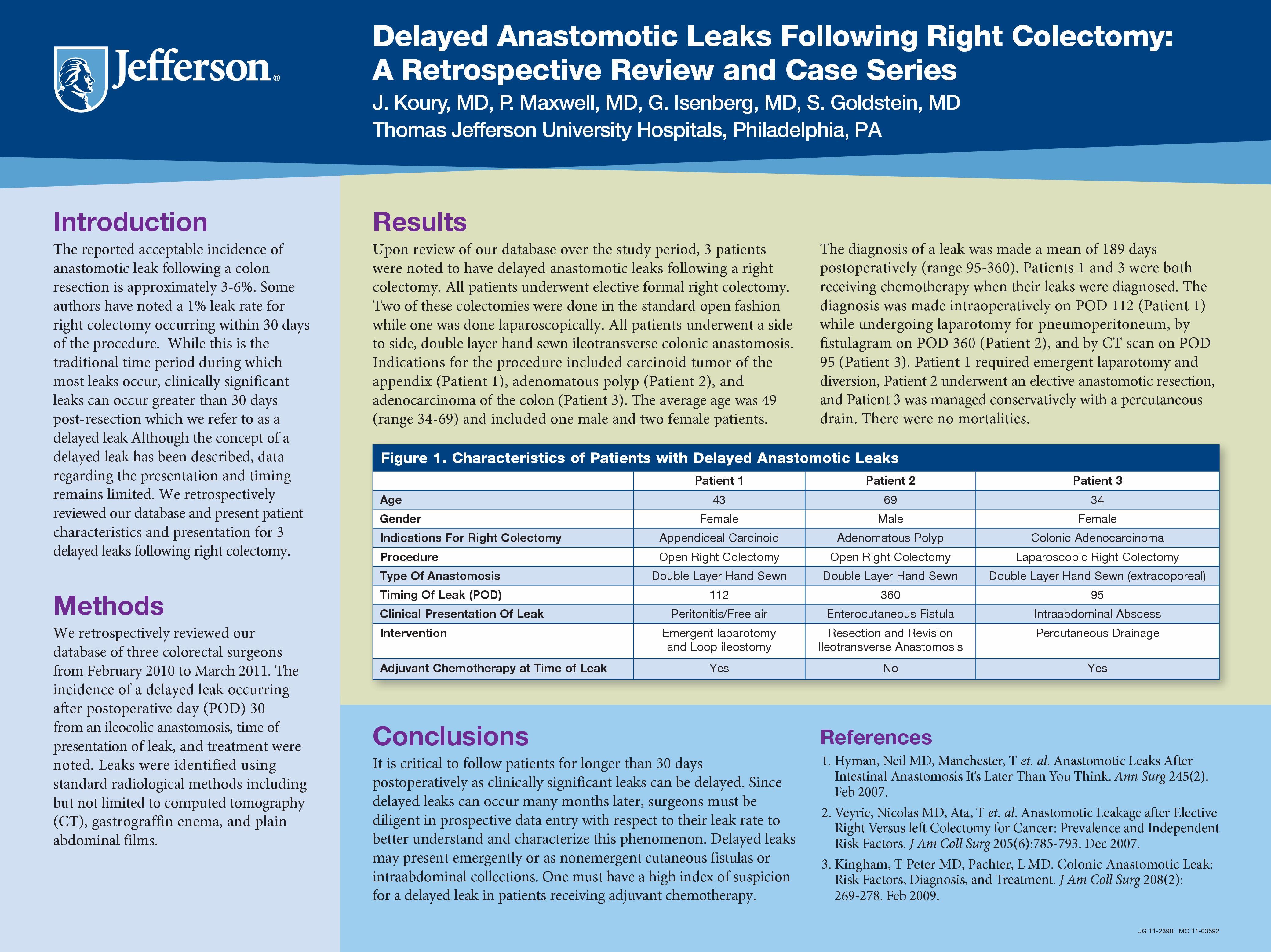
Results:Upon review of our database over the study period, 3 patients were noted to have delayed anastomotic leaks following a right colectomy. All patients underwent elective formal right colectomy. Two of these colectomies were done in the standard open fashion. All patients underwent a side to side, double layer hand sewn ileotransverse colonic anastomosis. Indications for the procedure included carcinoid tumor of the appendix, adenomatous polyp, and adenocarcinoma of the colon. The average age was 49 (range 34-69) and included one male and two female patients. The diagnosis was made a mean of 189 days postoperatively (range 95-360). The diagnosis was made by CT scan (POD 95), fistulagram (POD 360), and intraoperatively while undergoing laparotomy for pneumoperitoneum (POD 112). The two patients who leaked on POD 95 and 112 were both receiving adjuvant chemotherapy at the time their leaks were diagnosed. One patient (POD 112) required emergent laparotomy and diversion, one (POD 360) underwent an elective anastomotic resection, and one was managed conservatively with a percutaneous drain. There were no mortalities.
Conclusions: It is critical to follow patients for longer than 30 days postoperatively as clinically significant leaks can be delayed. Since delayed leaks can occur many months later, surgeons must be diligent in prospective data entry with respect to their leak rate to better understand and characterize this phenomenon. Delayed leaks may present emergently or as nonemergent cutaneous fistulas or intraabdominal collections. Lastly, one must have a high index of suspicion for a delayed leak in patients receiving adjuvant chemotherapy.
References:
Hyman, Neil MD, Manchester, T et. al. Anastomotic Leaks After Intestinal Anastomosis It’s Later Than You Think. Ann Surg 245(2). Feb 2007.
Veyrie, Nicolas MD, Ata, T et. al. Anastomotic Leakage after Elective Right Versus left Colectomy for Cancer : Prevalence and Independent Risk Factors. J Am Coll Surg 205(6):785-793. Dec 2007.
Kingham, T Peter MD, Pachter, L MD. Colonic Anastomotic Leak: Risk Factors, Diagnosis, and Treatment. J Am Coll Surg 208(2): 269-278. Feb 2009.
Session Number: Poster – Poster Presentations
Program Number: P052
View Poster