Brian Bassiri-Tehrani, MD1, Alex Wang2, William Harris2, Edmund Kessler, MD1. 1Lenox Hill Hospital, Zucker School of Medicine at Hofstra/Northwell, 2SUNY Downstate Medical Center
Intestinal atresia is a congenital malformation that occurs in 1 out of 5,000 live births, with equal incidence in males and females. One out of three infants with intestinal atresia are premature. The authors present a case of a 1-day-old female born at 38-weeks gestation via normal spontaneous vaginal delivery with bilious vomiting on the first day of life.
Antecedent pregnancy was normal and routine ultrasound screenings showed no evidence of any underlying pathology. Birth weight was 3360 grams, height/length was 83rd percentile, head circumference 54th percentile. Apgar score was 9 at 1 minute and 10 at 5 minutes. Birth physical exam was unremarkable without evidence of dysmorphic signs or features.
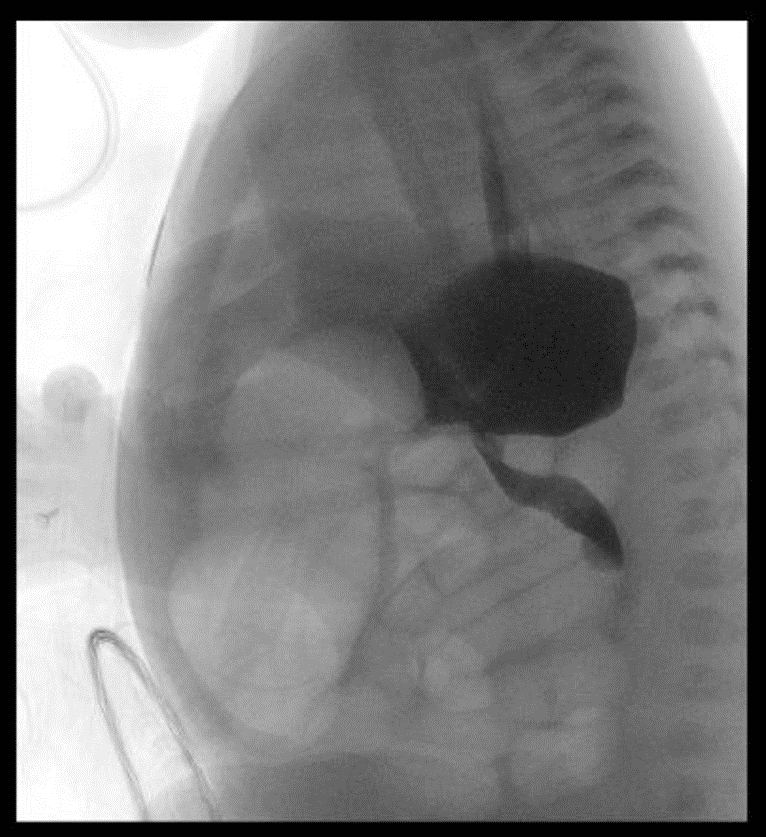
On day of life 1 the baby was tolerating her first breast feeds, however overnight the baby had bilious emesis and had yet to pass meconium. The patient’s abdomen was slightly more distended and tympanic. Plain film showed distended bowel. A replogle tube was placed. Vital signs were within the normal range and labs were unremarkable. Subsequently, an upper GI series was performed and showed a proximal small bowel obstruction.
A contrast enema was done and showed a patent rectum without evidence of a microcolon, Hirchsprung’s disease or malposition. The baby was then taken to the operating room on day of life 2 for an exploratory laparotomy.
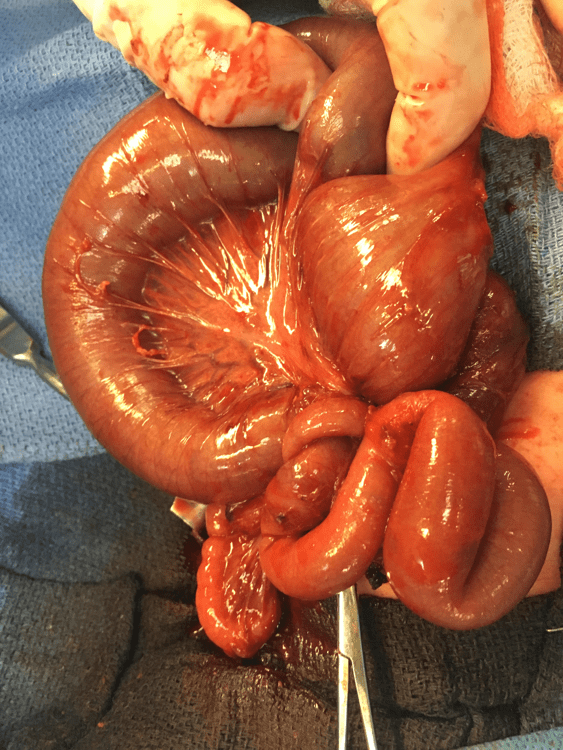
Upon entry into the peritoneal cavity, congenital adhesions were encountered and lysed. A midgut type IIIb intestinal atresia was found with an internal hernia through a mesenteric defect. A 15cm segmental bowel resection was performed with a single layer hand sewn anastomosis was performed. Postoperatively, the baby was extubated and placed on nasal cannula with the replogle in place.
The baby required parental nutrition for weeks after surgery due to inability to consistently tolerate a PO diet despite repeated upper GI films ruling out a mechanical obstruction. Therefore, on post op day 20, the baby started a 5 day course of erythromycin to promote GI motility. After the start of erythromycin, the baby was started on feeds and was gradually advanced with good tolerance. On post op day 37, the baby continue to tolerate a PO diet and was reintroduced to expressed breast milk. The baby was reliably tolerating a home breast feeding schedule by post op day 39. On post op day 41 the baby was discharged home.
.png)
.png)
.png)


Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 94479
Program Number: P644
Presentation Session: Poster Session (Non CME)
Presentation Type: Poster