Piotr Walega, MD PhD, Jakob Kenig, MD, Piotr Richter, Prof, Wojciech Nowak, Prof. Jagiellonian University Collegium Medicum
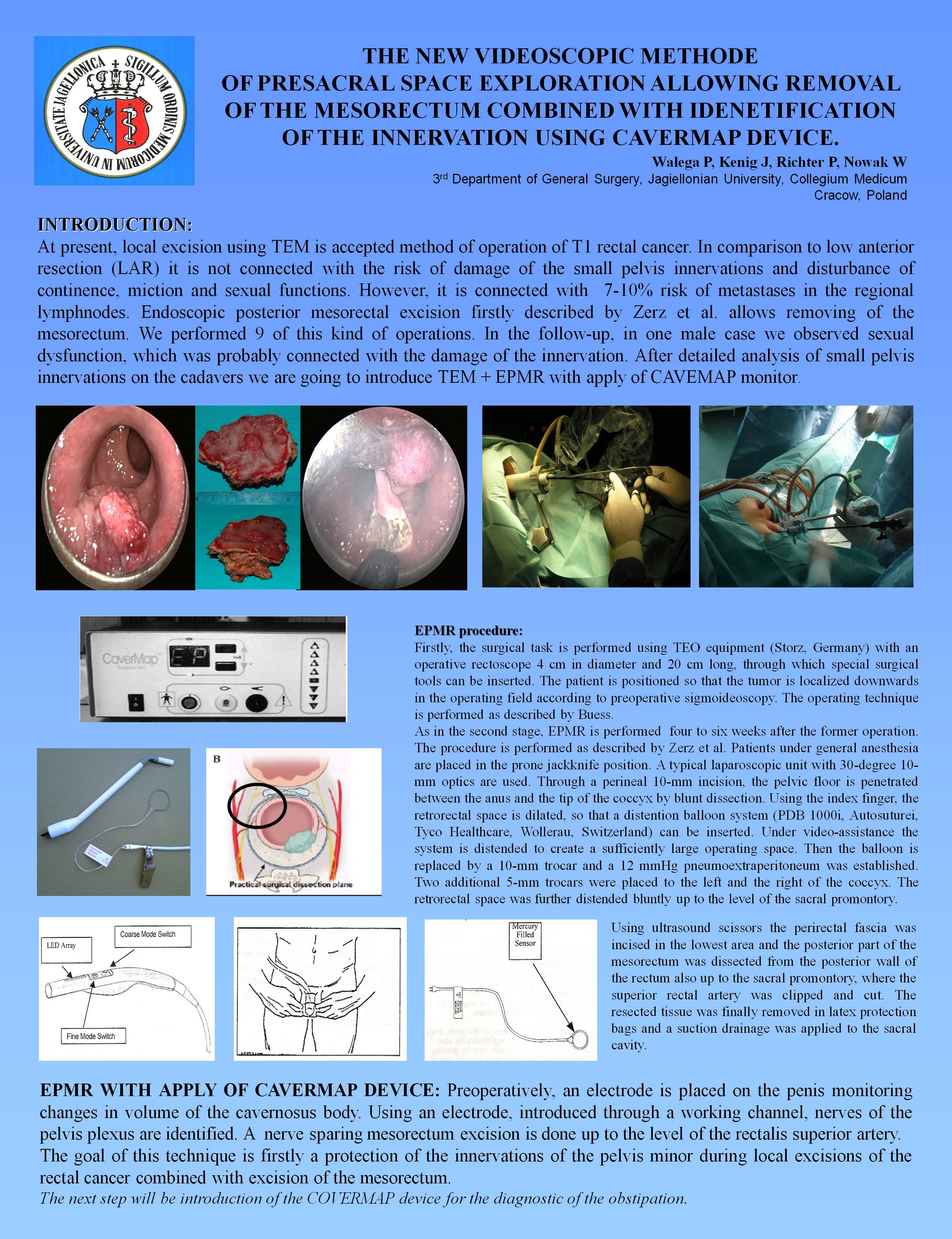
At present, local excision using TEM is accepted method of operation of T1 rectal cancer. However, it is connected with 7-10% risk of metastases in the regional lymph nodes. Endoscopic posterior mesorectal excision, firstly described by Zerz et al., allows removing mesorectum. We performed 9 of this kind of operations. In the follow-up, in one male case we observed sexual dysfunction, which was probably connected with the damage of the innervation. After detailed analysis of small pelvis innervations on the cadavers we are going to introduce TEM + EPMR with apply of CAVEMAP monitor. The goal of the project is minimal invasive removal of the tumor with lymph nodes with simultaneous assessment and protection of the innervations. Firstly, the surgical task is performed using TEO equipment (Storz, Germany) with an operative rectoscope 4 cm in diameter and 20 cm long, through which special surgical tools can be inserted. The patient is positioned so that the tumor is localized downwards in the operating field according to preoperative sigmoideoscopy. The operating technique is performed as described by Buess. As in the second stage, EPMR is performed four to six weeks after the former operation. The procedure is performed as described by Zerz et al. Patients under general anesthesia are placed in the prone jackknife position. A typical laparoscopic unit with 30-degree 10-mm optics are used. Through a perineal 10-mm incision, the pelvic floor is penetrated between the anus and the tip of the coccyx by blunt dissection. Using the index finger, the retrorectal space is dilated, so that a distention balloon system (PDB 1000i, Autosuturei, Tyco Healthcare, Wollerau, Switzerland) can be inserted. Under video-assistance the system is distended to create a sufficiently large operating space. Then the balloon is replaced by a 10-mm trocar and a 12 mmHg pneumoextraperitoneum was established. Two additional 5-mm trocars were placed to the left and the right of the coccyx. The retrorectal space was further distended bluntly up to the level of the sacral promontory. Using ultrasound scissors the perirectal fascia was incised in the lowest area and the posterior part of the mesorectum was dissected from the posterior wall of the rectum also up to the sacral promontory, where the superior rectal artery was clipped and cut. The resected tissue was finally removed in latex protection bags and a suction drainage was applied to the sacral cavity. EPMR with apply of Cavermap device: Preoperatively, an electrode is placed on the penis monitoring changes in volume of the cavernosus body. Using an electrode, introduced through a working channel, nerves of the pelvis plexus are identified. A nerve sparing mesorectum excision is done up to the level of the rectalis superior artery. The goal of this technique is firstly a protection of the innervations of the pelvis minor during local excisions of the rectal cancer combined with excision of the mesorectum. The next step will be introduction of the COVERMAP device for the diagnostic of the obstipation.
Session: Emerging Technology Poster
Program Number: ETP104
View Poster
{kind=link}