Adam Young, PhD1, Collin E. M Brathwaite, MD, FACS, FASMBS2, Thomas W Gilbert, PhD1. 1ACell Inc, 2NYU Winthrop Hospital
Mesh reinforcement of hiatal hernia repairs has been previously shown to reduce recurrence rates compared to primary repair alone, however, the risk of esophageal erosion and stricture limit the utility of many materials for this application. Recent publications have described early clinical successes in using urinary bladder matrix (UBM) for reinforcement of hiatal and ventral hernia repairs. In this study, a porcine model of laparoscopic hiatal hernia repair was utilized to compare the tissue responses between non-reinforced primary repairs to repairs reinforced with a “U-shape” surgical graft composed entirely of UBM.
Hiatal hernias were simulated in pigs by laparoscopically dissecting the phrenoesophageal ligament and separating the left and right crus. The defect was then repaired by suturing the crura with an EndoStitch device. Five pigs were then closed with only this primary suture repair, while another five pigs received reinforcement of the primary repair with a UBM surgical graft that was pre-fashioned into a “U-shape” configuration (Fig 1a,b). All animals were survived for two months, at which point the animals were evaluated endoscopically for esophageal stricture or erosion. The repair site was then harvested for histological evaluation.
All animals recovered from surgery and gained weight with no signs of dysphagia. At two months post-operatively, endoscopic evaluation showed slight stricture at the GE junction in both reinforced and non-reinforced animals as a result of the procedure, but no evidence of erosion. Adhesions to the underlying viscera were minimal and similar in both groups as well. Histologic evaluation found only minimal evidence of the UBM device remaining, with the rest of the device having remodeled into tissue that was largely indistinguishable from the surrounding diaphragmatic tissue (Fig 1c). An increase in granulation tissue was noted in the reinforced animals compared to the non-reinforced controls.
This study highlights the safety of a UBM-derived device in the laparoscopic reinforcement of hiatal hernia repairs. The device was completely remodeled into site appropriate tissue that minimized the risk of stricture or erosion of the esophagus. Although this is an early time point, the deposition of new granulation tissue and absence of complications provides histologic evidence for the successful clinical outcomes that have been previously published for UBM devices in the reinforcement of hiatal hernia repairs.
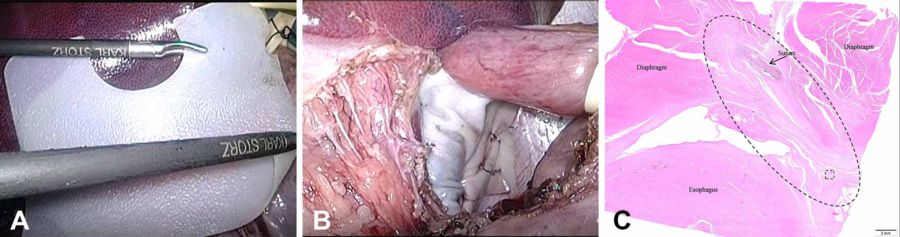
Figure 1: U-shaped UBM device was inserted laparoscopically without damage (A) and tacked to the diaphragm (B). At 2 months, histology (C) showed UBM (oval) had remodeled without damaging surrounding anatomy.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 93811
Program Number: P533
Presentation Session: Poster Session (Non CME)
Presentation Type: Poster