Kunihito Suzuki, MD, Yosuke Izumi, MD, PhD, Tairo Ryotokuji, MD, Akinori Miura, MD, PhD, Tsuyoshi Kato, MD, Michiyo Tokura, MD
Tokyo Metropolitan Cancer and Infectious diseases Center, Komagome Hospital
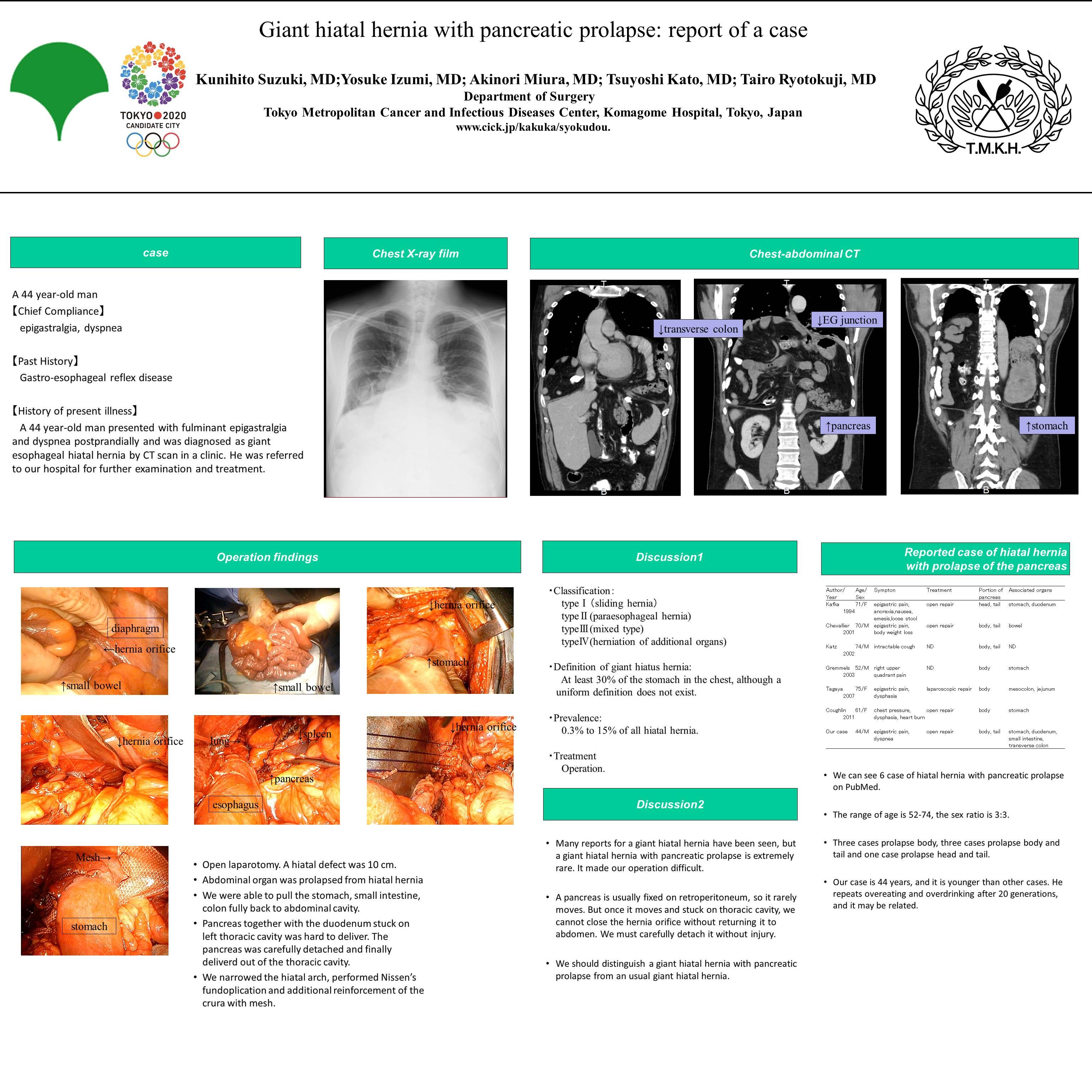
44 year-old man presented with fulminant epigastralgia and dypnea postprandially and was diagnosed as giant esophageal hiatal hernia by CT scan in a clinic. He was referred to our hospital for further examination and treatment. CT scan showed whole stomach, almost whole small intestine, right and transverse colon and pancreas prolapsed above diaphragm, and type IV esophageal hiatal hernia was diagnosed.We performed elective open hiatal hernia repair. Operative findings were a giant hiatal hernia, defined as a hiatal defect 10 cm, massive gastrointestinal prolapse and winding esophagus. We were able to pull the stomach, small intestine, colon fully back to abdominal cavity relatively easily, but pancreas together with the duodenum stuck on left thoracic cavity was hard to deliver. The pancreas was carefully detached and finally deliverd out of the thoracic cavity. We narrowed the hiatal arch, performed Nissen’s fundoplication and additional reinforcement of the crura with mesh. A giant hiatal hernia is a hernia that includes at least 30% of the stomach in the chest, although a uniform definition does not exist. Most commonly, a giant hiatal hernia is a type III hernia with a sliding and paraesophageal component. A giant hiatal hernia has a risk of volvulus and strangulation of the stomach though often undetected for years before this life-threatening event.
Many reports for a giant hiatal hernia have been seen, but a giant hiatal hernia with pancreatic prolapse is extremely rare and delivering pancreas was thought to be most difficult point during the operative procedure.
Session: Poster Presentation
Program Number: P241