Calvin Lyons, MD, David Goldfarb, MD, Brian Miles, MD, Rohan Joseph, MD, Richard Link, MD, Barbara L Bass, MD, Brian J Dunkin, MD. The Methodist Institute for Technology, Innovation, and Education
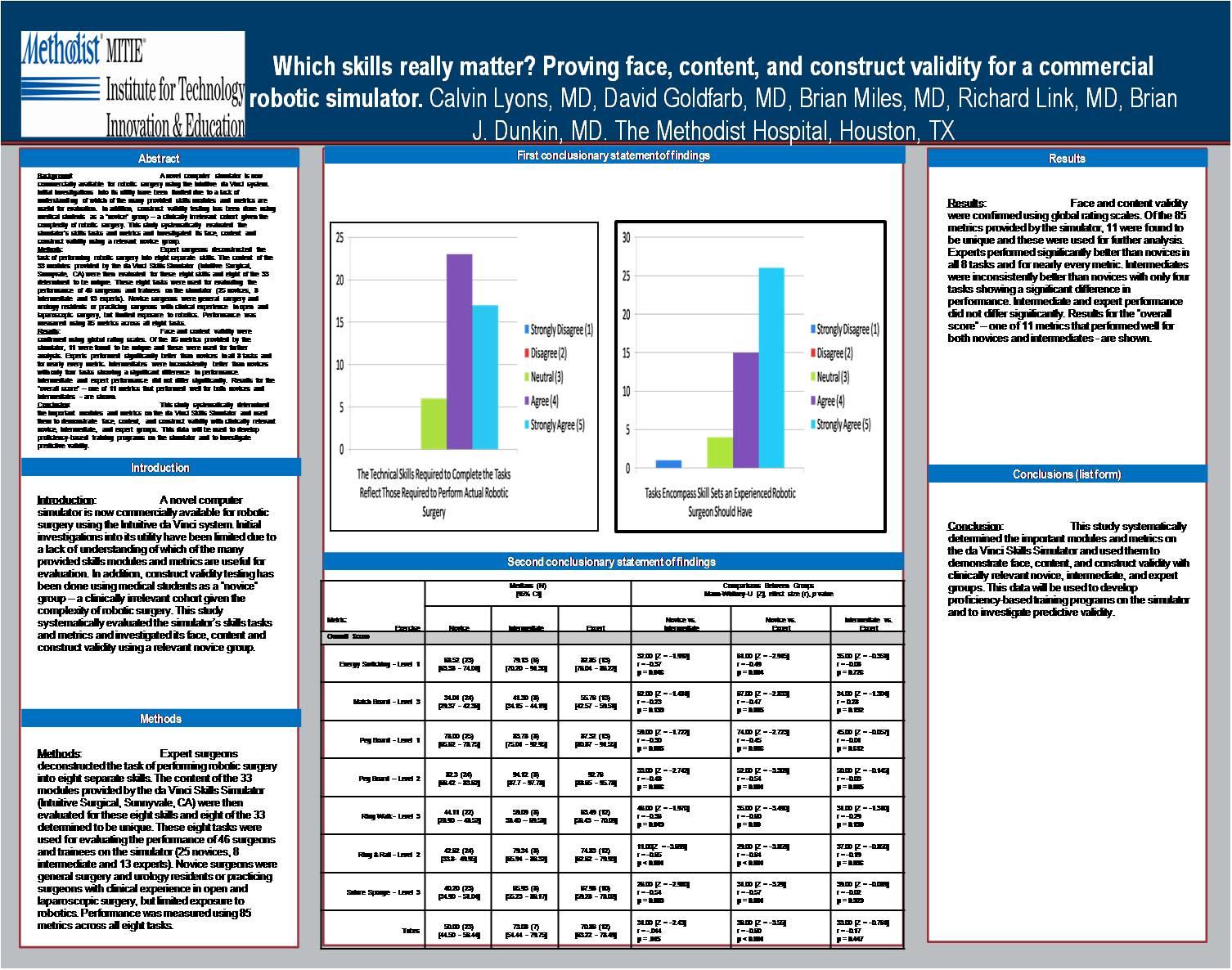
Background: A novel computer simulator is commercially available for robotic surgery. Initial validation studies have been limited due to a lack of understanding of which of the many provided skills modules and metrics are useful for evaluation. Construct validation studies are further limited in that medical students are used as a “novice” group – a clinically irrelevant cohort given the complexity of robotic surgery. This study systematically evaluated the simulator’s skills modules and metrics and investigated its face, content and construct validity using a relevant novice group.
Methods: Expert surgeons deconstructed robotic surgery into eight separate skills. The content of the 33 modules on the da Vinci Skills Simulator (Intuitive Surgical) were evaluated for these eight skills and eight of the 33 determined to be unique. These eight tasks were then used to evaluate the performance of 46 surgeons and trainees (25 novices, 8 intermediate and 13 experts). Novice surgeons were mid-level general surgery and urology residents or practicing surgeons with clinical experience in open and laparoscopic surgery, but limited exposure to robotics.
Results: Face and content validity were confirmed using global rating scales. Of the 85 metrics provided by the simulator, 11 were found to be unique. Experts performed significantly better than novices in all 8 tasks and for nearly every metric. Intermediates were inconsistently better than novices with only four metrics showing a significant difference in performance. Intermediate and expert performance did not differ significantly. Results for the “overall score” – one of 11 metrics that performed well – are shown.
| Overall Score | Novice | Intermed | Expert | Novice vs. Expert |
Novice vs. Intermed |
Intermed vs. Expert |
|---|---|---|---|---|---|---|
| Energy | 68 [63 – 74] |
79 [70 – 91] |
83 [76 – 86] |
p = 0.004 | p = 0.046 | p = 0.726 |
| Match Board 3 | 34 [29 – 42] |
41 [34 – 44] |
55 [42 – 59] |
p = 0.005 | p = 0.139 | p = 0.192 |
| Peg 1 | 78 [66 – 79] |
83 [75 – 92] |
87 [81 – 92] |
p = 0.006 | p = 0.085 | p = 0.612 |
| Peg 2 | 82 [66 – 84] |
94 [88 – 98] |
93 [89 – 96] |
p = 0.001 | p = 0.006 | p = 0.885 |
| Ring Walk 3 | 44 [29 – 49] |
59 [38 – 70] |
63 [56 – 70] |
p = 0.001 | p = 0.049 | p = 0.190 |
| Ring Rail 2 | 43 [34 – 50] |
79 [66 – 86] |
75 [63 – 80] |
p < 0.001 | p < 0.001 | p = 0.096 |
| Suture Sponge | 40 [35 – 51] |
66 [55 – 86] |
68 [59 – 78] |
p = 0.001 | p = 0.003 | p = 0.929 |
| Tubes | 50 [45 – 56] |
73 [54 – 80] |
71 [63 – 78] |
p < 0.001 | p = .015 | p = 0.447 |
Conclusion: This study systematically determined the important modules and metrics on the da Vinci Simulator and used them to demonstrate face, content, and construct validity with clinically relevant novice, intermediate, and expert groups. The results will be used to develop proficiency-based training programs and to investigate predictive validity.
Session Number: Poster – Poster Presentations
Program Number: P173
View Poster