Background: Modern medical informatics is changing the way physicians practice and how clinical research is conducted. The appropriate utilization of a clinical database, electronic medical records (EMR), and other health related software can improve patient care and offer the opportunity for practice analysis and HIPAA compliant research. With IRB approval, clinician researchers can use this technology to prospectively enroll consenting subjects into a database compliant with the Belmont Report (45 CFR §46.111a3).
Objectives: The secure electronic clinical database will prospectively accrue consenting subjects. De-identified patients treated retrospectively (over the past ten years) will also be added to the clinical database. By analyzing the database, clinicians will compare their results to national averages and report significant findings to peer reviewed journals. This database will also securely accumulate past and current research-project data and link this data to clinical outcomes stored within the database.
Database Strategy: Making the most of modern health-software can streamline subject and data accrual. For example, once a subject is added to a database, data points from the EMR can be automatically downloaded into the database. Retrospective subjects are available for immediate input. Analyzing retrospective outcomes can reveal unique discrepancies or complexities. These issues can be further explored in detail by tailor-designing prospective accrual data points. This will improve own-practice outcomes and the validity of database reporting. Including data from other research projects will improve database power and highlight important clinical outcomes associated with that research data.
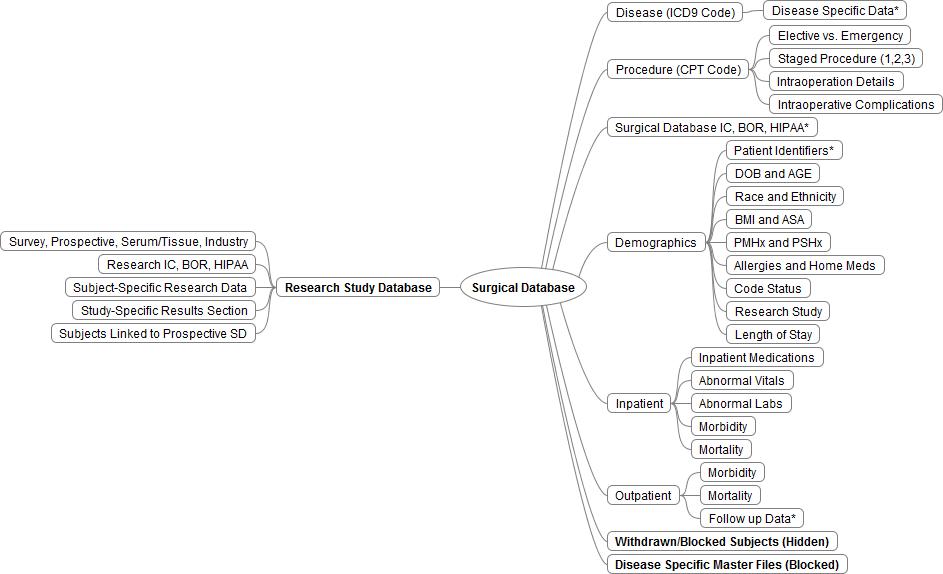
Database Design: The database will be stratified based on disease (ICD9 Code) and procedure (CPT Code). The design includes disease and procedure specific data, demographics, inpatient and follow-up data fields (Figure 1). Prospective participants will have viewable patient identifiers and a section that displays their informed consent documentation while the retrospective subjects will not. Excel files used to create the retrospective database will be stored but blocked while withdrawn subjects will be removed and blocked. The research database will be stratified according to current or past research projects. The research database will also link to the clinical database, store consenting documentation, research data and study results.
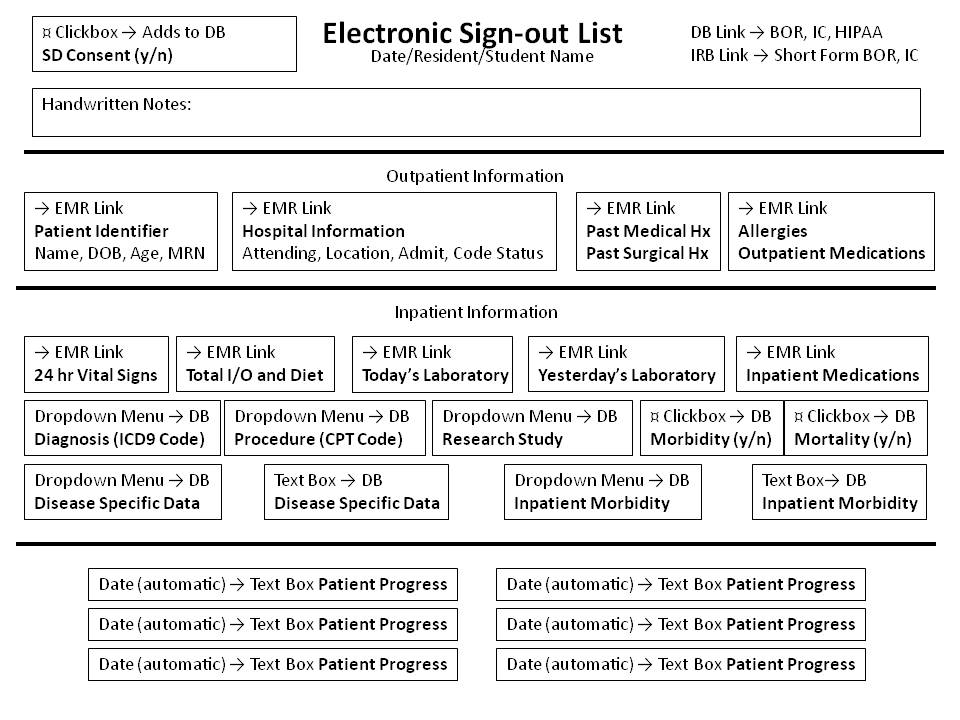
Database Software and Security: Hospital informational technology (IT) can build a secure clinical electronic database designed upon departmental specifications. IT grants, monitors and secures database access to protect private medical information. IT can also create database links to the EMR and other health-software. An important link is to an electronic sign-out list that can streamline patient/data accrual at point of care. This program eases access to consenting documentation and eliminates the need for database login (Figure 2).
Analysis and Reporting: Quarterly analysis of accrued data can be compared to countrywide standards and emphasize areas that need improvement. Analysis may even yield clinically significant findings worthy of publication. National healthcare reimbursement is trending towards pay for performance and away from fee for service. The clinician can prepare to overcome these changes by employing available technology that utilizes a clinical database.