Naoshi Kubo, Katsunobu Sakurai, Hiroaki Tanaka, Kazuya Muguruma, Hitoshi Nagahara, Eiji Noda, Kiyoshi Maeda, Masakazu Yashiro, Nobuya Yamada, Masaichi Ohira, Kosei Hirakawa. Department of Surgical Oncology, Graduate school of medicine, Osaka-City University
Background
The thoracoscopic esopagectomy for esophageal cancer has been reported as minimally invasive with regard to less thoracic wall injury and decreased respiratory function. We had inducted thoracoscopic esophagectomy with minithoracotomy at left lateral position (TEL) in September 1999 and TEL were consectively performed in about 100 cases. Additionaly, thoracoscopic esophagectomy in semi prone position (TEP) was conducted in April 2010. This procedures included upper mediastinum lymph-adenectomy in left decubitus position and lower mediastinum lymph-adenectmy in prone position. Patients was placed on the surgical table in left lateral-prone position. Surgical table can be tilted to prone or lateral position immediately . The CO2 insufflation at a pressure of 7mmHg was established during operation and good surgical exposure was obtained because of gravity and lung collapse. We retrospectively compared surgical outcomes in 15 TEP cases to those of 28 TEL cases as a historical control.
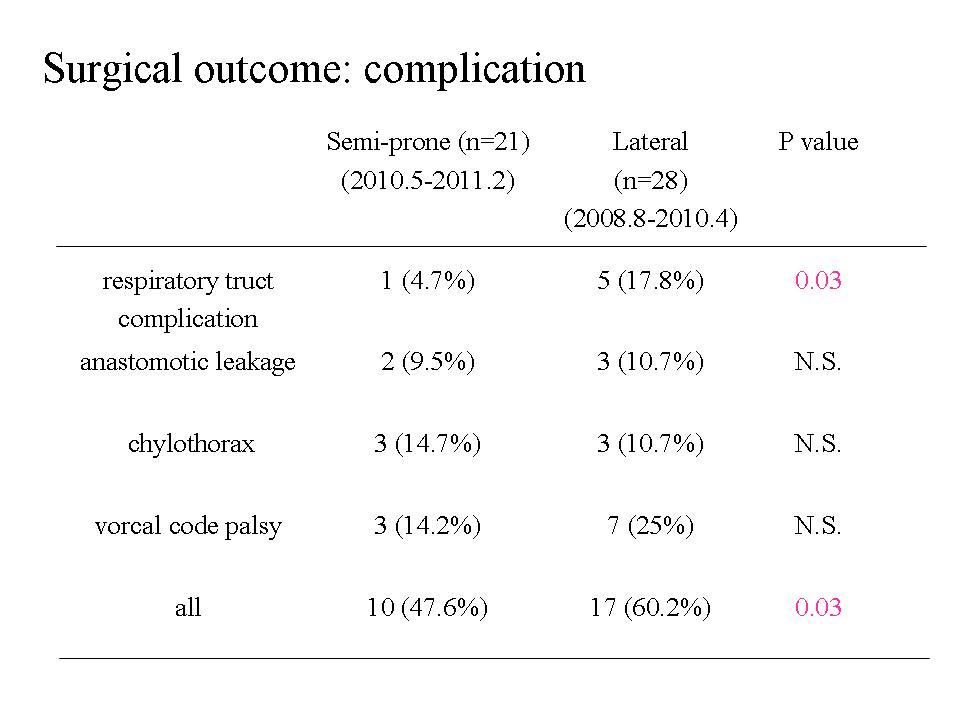
(Result) There were no differences between the two groups in patients background (age, gender, tumor stage, tumor location). The mean blood loss during thoracoscopic portion were significantly lesser in TEP than TEL (123 versus 285 min, p = 0.02). The incidence of pulmonaly complication was significantly lesser in TEP than in TEL. The levels of C reactive protein on postoperative day1 and 2 were significantly lower in TEP patients than TEL patients. (conclusion) TEP was less invasive procedure compared toTEL.
Session Number: Poster – Poster Presentations
Program Number: P525
View Poster