Prateek K Gupta, MD, Himani Gupta, MD, R. Armour Forse, MD PhD. Creighton University
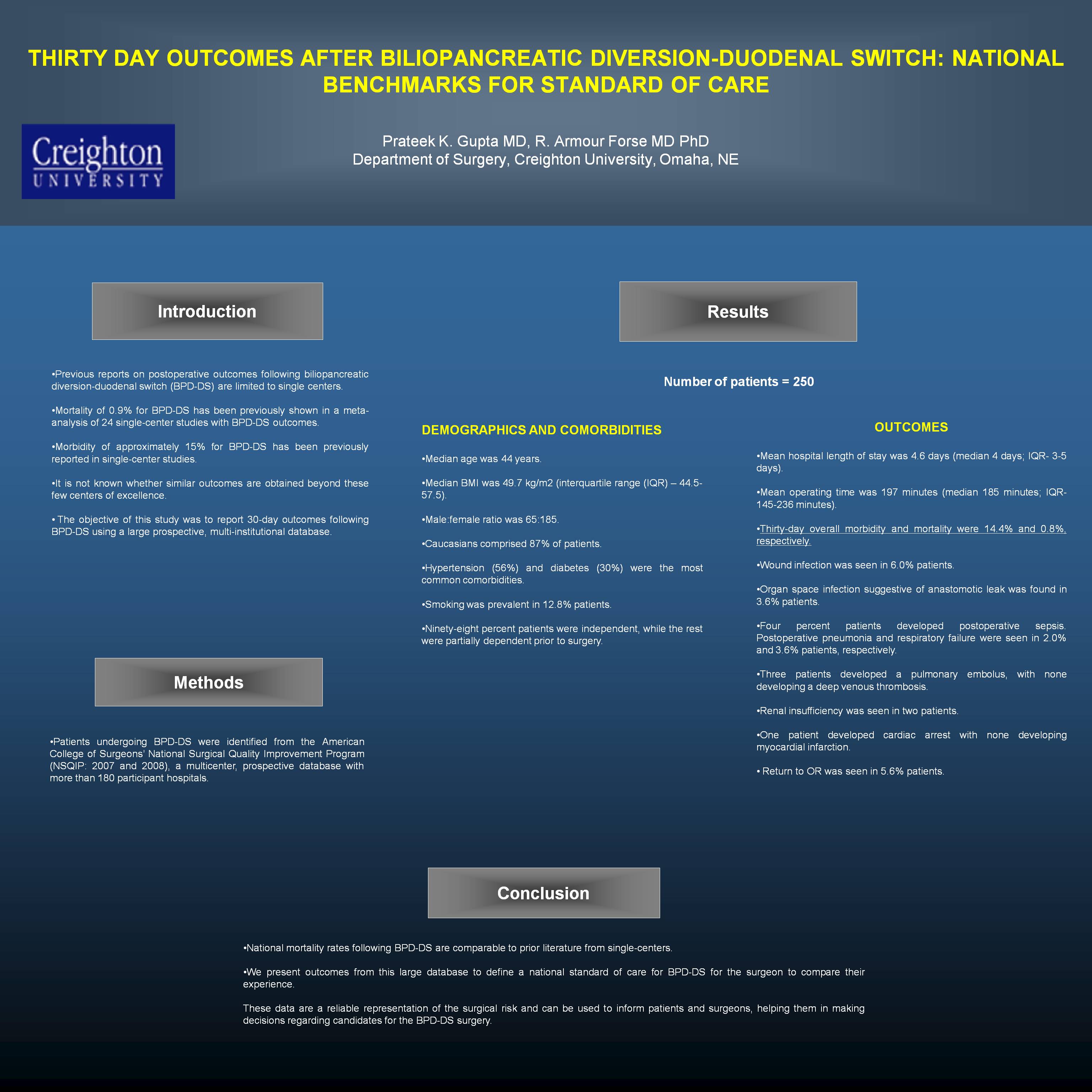
Objectives: Previous reports on postoperative outcomes following biliopancreatic diversion-duodenal switch (BPD-DS) are limited to single centers. Mortality of 0.9% for BPD-DS has been previously shown in a meta-analysis of 24 single-center studies with BPD-DS outcomes. It is not known whether similar outcomes are obtained beyond these few centers of excellence. The objective of this study was to report 30-day outcomes following BPD-DS using a large prospective, multi-institutional database.
Methods: Patients undergoing BPD-DS were identified from the American College of Surgeons’ National Surgical Quality Improvement Program (NSQIP: 2007 and 2008), a multicenter, prospective database with more than 180 participant hospitals.
Results: Two hundred fifty patients undergoing BPD-DS were identified. Median age was 44 years. Median BMI was 49.7 kg/m² (interquartile range (IQR) – 44.5-57.5). Male:female ratio was 65:185. Caucasians comprised 87% of patients. Hypertension (56%) and diabetes (30%) were the most common comorbidities. Smoking was prevalent in12.8% patients. Ninety-eight percent patients were totally dependent, while the rest were partially dependent prior to surgery. Mean hospital length of stay was 4.6 days (median 4 days; IQR- 3-5 days). Mean operating time was 197 minutes (median 185 minutes; IQR- 145-236 minutes). Thirty-day overall morbidity and mortality were 14.4% and 0.8%, respectively. Wound infection was seen in 6.0% patients. Organ space infection suggestive of anastomotic leak was found in 3.6% patients. Four percent patients developed postoperative sepsis. Postoperative pneumonia and respiratory failure were seen in 2.0% and 3.6% patients, respectively. Three patients developed a pulmonary embolus, with none developing a deep venous thrombosis. Renal insufficiency was seen in two patients. One patient developed cardiac arrest with none developing myocardial infarction. Return to OR was seen in 5.6% patients.
Conclusion: National mortality rates following BPD-DS are comparable to prior literature from single-centers. We present outcomes from this large database to define a national standard of care for BPD-DS for the surgeon to compare their experience. This data could be utilized by third party interests, and surgeons should be aware of benchmarks to ensure their outcomes are in the national norm.
Session: Poster
Program Number: P043
View Poster
{kind=link}