Ambar Banerjee, MD, Yi Ding, BS, Nilay Shah, MD, Dean J Mikami, MD, Bradley J Needleman, MD. Center for Minimally Invasive Surgery, Division of General and Gastrointestinal Surgery, The Ohio State University, Columbus, Ohio
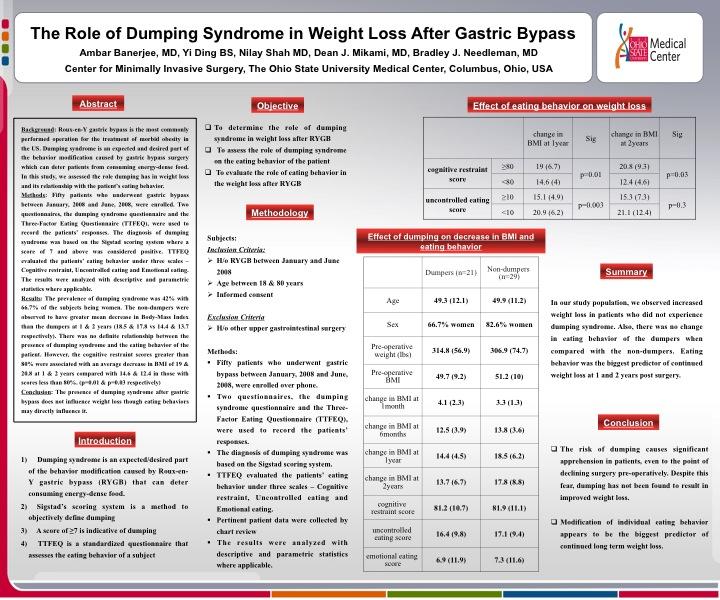
Background: Roux-en-Y gastric bypass (RNYGB) is the most commonly performed operation for the treatment of morbid obesity in the US. Dumping syndrome is an expected side effect that may be desirable as part of the behavior modification caused by gastric bypass surgery, which can deter patients from consuming energy-dense food. In this study, we assessed the role dumping has in weight loss and its relationship with the patient’s eating behavior.
Methods: After obtaining Institutional Review Board approval, fifty patients who underwent gastric bypass between January 2008 and June 2008 were enrolled. Two questionnaires, the dumping syndrome questionnaire and the revised Three-Factor Eating Questionnaire (TFEQ-R18), were administered to the patients. The diagnosis of dumping syndrome was based on the Sigstad scoring system where a score of 7 and above was considered positive. TFEQ-R18 evaluated the patients’ eating behavior under three scales – Cognitive restraint, Uncontrolled eating and Emotional eating. The patients were asked about dumping syndrome symptoms, usually following sweet ingestion, at three points in time – preoperative, immediate postoperative, and 2 years post surgery. TFEQ-R18 was completed on the basis of their diet at the time of execution of the questionnaire. The medical records of the enrolled patients were reviewed to collect pertinent data on demographics including their body weights and body mass index (BMI). BMI loss was calculated at 1 month, 6 months, 1 year and at 2 years post surgery. The results were analyzed with descriptive and parametric statistics, where applicable.
Results: The prevalence of dumping syndrome in our study population was 42%. Twelve of these 21 patients (57.1%) complained of early dumping only, while 9 patients experienced symptoms of both early and late dumping. All of the patients experienced resolution of the symptoms between 1 and 2 years post RNYGB. At one month post RNYGB, the dumpers lost an average of 4.1 kg/m2 in their BMI compared to 3.3 kg/m2 in non-dumpers. (p=0.29) However, at the remaining points of observation, the non-dumpers were observed to suffer a greater decrease in BMI than the dumpers: 13.8 kg/m2 vs 12.5 kg/m2at 6 months (p=0.39), 18.5 kg/m2 vs 14.4 kg/m2 at 1 year (p=0.57) and 17.8 kg/m2 vs 13.7 kg/m2 at 2 years post surgery (p=0.39). There was no definite relationship between the presence of dumping syndrome and the eating behavior of the patient. However, patients with cognitive restraint scores greater than 80% were associated with an average decrease in BMI of 19 & 20.8 kg/m2 at 1 & 2 years compared with 14.6 & 12.4 kg/m2 in those with scores less than 80%. (p=0.01 & p=0.03 respectively) Similarly, those who showed low uncontrolled eating scores (<10) experienced greater decrease in their BMI at 6 months (15.7 vs. 12.4, p=0.01) and 1 year (20.9 vs 15.1, p=0.003).
Conclusion: The presence of dumping syndrome after RNYGB does not influence weight loss. However, eating behaviors, as measured by the TFEQ-R18, may directly influence weight loss. Modification of individual eating behavior appears to be the biggest predictor of continued long term weight loss.
Session Number: Poster – Poster Presentations
Program Number: P464
View Poster