Sumio Matsumoto, PhD, Hiromi Tokumura, Dr, Yuichi Yamashita, Professor, Taizo Kimura, DMsc, Toshiyuki Mori, Professor, Fumio Konishi, Professor, Seigo Kitano, Professor, Masaki Kitajima, Professor. ESSQS Committee of the Japan Society for Endoscopic Surgery
Purpose: The Japan Society for Endoscopic Surgery (JSES) started Endoscopic Surgical Skill Qualification (ESSQS) in 2004, and carried out seven examinations up to 2010. We reported these results and consideration as to consensus meeting needed.
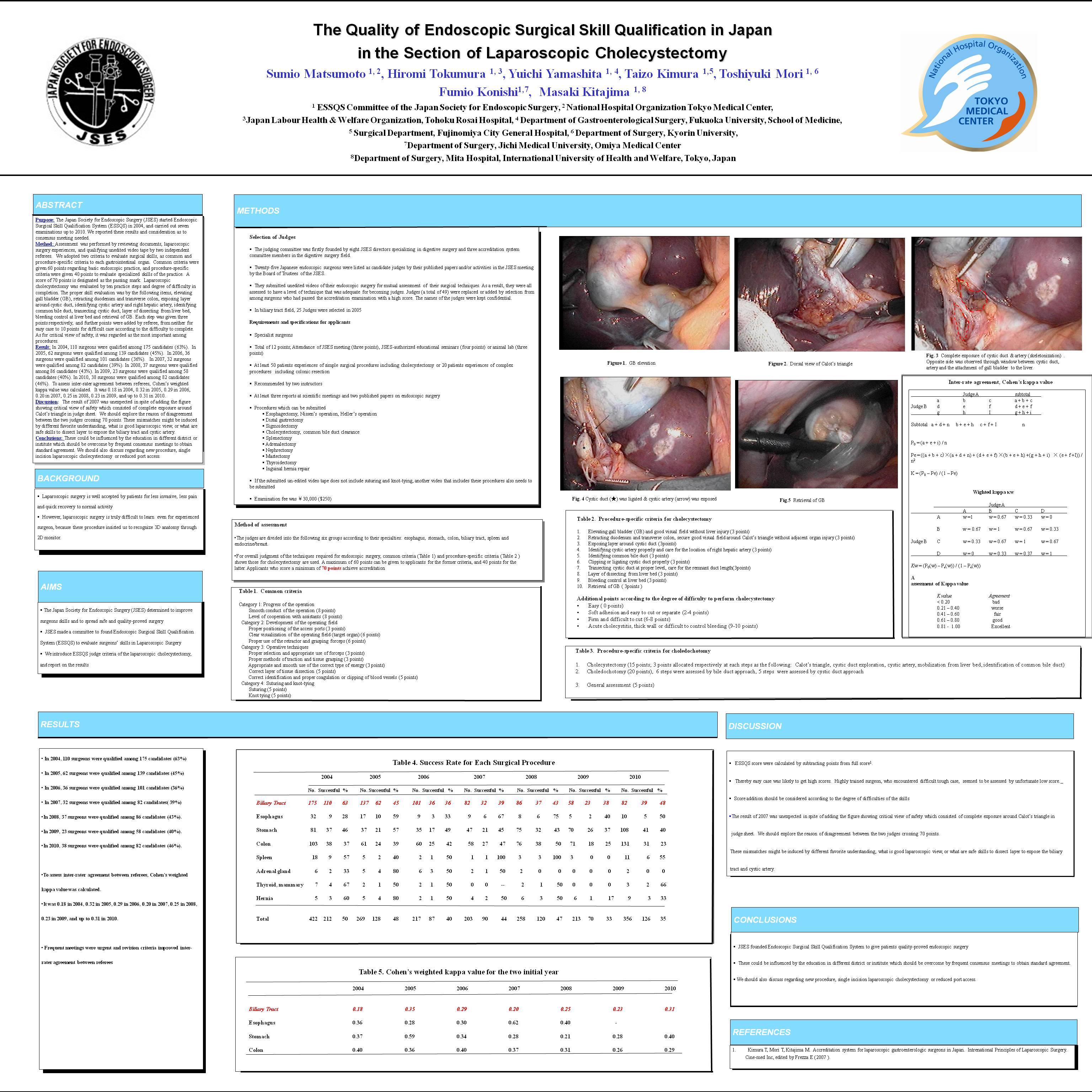
Methods: Assessment was performed by reviewing documents, laparoscopic surgery experiences, and qualifying unedited video tape by two independent referees. We adopted two criteria to evaluate surgical skills, as common and procedure-specific criteria to each gastrointestinal organ. Common criteria were given 60 points regarding basic endoscopic practice, and procedure-specific criteria were given 40 points to evaluate specialized skills of the practice. A score of 70 points is designated as the passing mark. Laparoscopic cholecystectomy was evaluated by ten practice steps and degree of difficulty in completion. The proper skill evaluation was by the following items, elevating gall bladder (GB), retracting duodenum and transverse colon, exposing layer around cystic duct, identifying cystic artery and right hepatic artery, identifying common bile duct, transecting cystic duct, layer of dissecting from liver bed, bleeding control at liver bed and retrieval of GB. Each step was given three points respectively, and further points were added by referee, from neither for easy case to 10 points for difficult case according to the difficulty to complete. As for critical view of safety, it was regarded as the most important among procedures.
Results: In 2004, 110 surgeons were qualified among 175 candidates (63%). In 2005, 62 surgeons were qualified among 139 candidates (45%). In 2006, 36 surgeons were qualified among 101 candidates (36%). In 2007, 32 surgeons were qualified among 82 candidates (39%). In 2008, 37 surgeons were qualified among 86 candidates (43%). In 2009, 23 surgeons were qualified among 58 candidates (40%). In 2010, 38 surgeons were qualified among 82 candidates (46%). To assess inter-rater agreement between referees, Cohen’s weighted kappa value was calculated. It was 0.18 in 2004, 0.32 in 2005, 0.29 in 2006, 0.20 in 2007, 0.25 in 2008, 0.23 in 2009, and up to 0.31 in 2010.
Discussion: The result of 2007 was unexpected in spite of adding the figure showing critical view of safety which consisted of complete exposure around Calot’s triangle in judge sheet. We should explore the reason of disagreement between the two judges crossing 70 points. These mismatches might be induced by different favorite understanding, what is good laparoscopic view, or what are safe skills to dissect layer to expose the biliary tract and cystic artery.
Conclusion: These could be influenced by the education in different district or institute which should be overcome by frequent consensus meetings to obtain standard agreement. We should also discuss regarding new procedure, single incision laparoscopic cholecystectomy or reduced port access.
Session Number: Poster – Poster Presentations
Program Number: P523
View Poster