Roel Hompes, MD, Frederic Ris, MD, Christopher Cunningham, FRCS, Neil Mortensen, FRCS, Ronan Cahill, MD. Department of colorectal surgery, John radcliffe hospitals, Oxford
Objective: The role for Transanal Endoscopic Microsurgery (TEM) in the treatment of rectal tumours is progressing. However, the cost and complex learning curve limit widespread utilisation by colorectal surgeons. Single port laparoscopic tools and principles are transferable to transanal work and various adapted approaches are being reported. Here we describe our initial clinical experience and preliminary data with a new and cost-effective technique for transanal work.
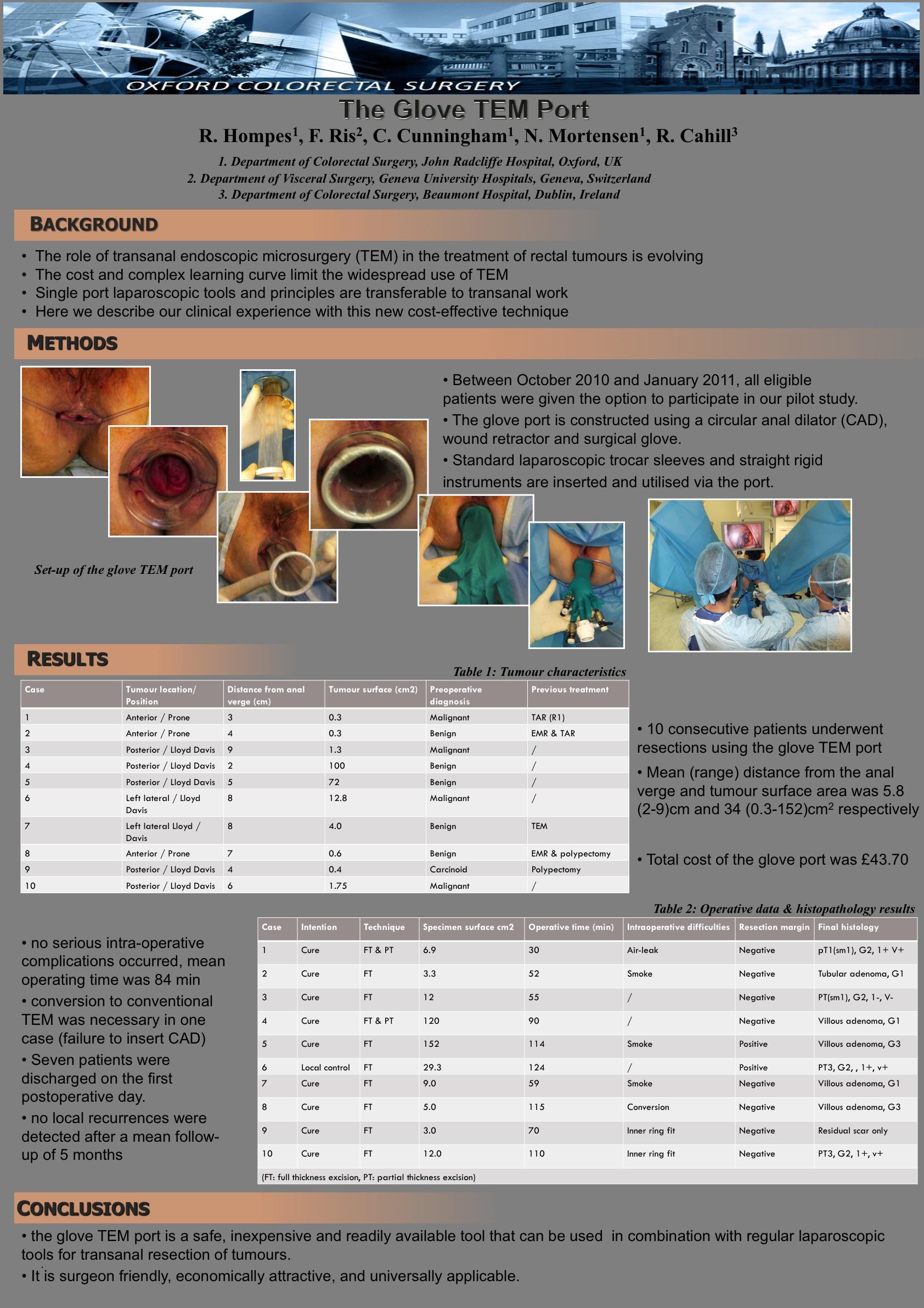
Materials and Methods: Between October 2010 and January 2011, all patients eligible for TEM were offered the option to participate in our pilot study. The glove TEM port is constructed on table by using a circular anal dilator (CAD), wound retractor and surgical glove into which standard laparoscopic trocar sleeves and straight rigid instruments are inserted.
Results: Initial preliminary work standardised both set-up and application of the apparatus and confirmed it outperformed commercially available counterparts in this application with regard to stability, instrument manoeuvreability and range of movement. With this new access modality, ten consecutive patients underwent resection of benign (n=6) or malignant (n=4) rectal tumours. The mean (range) distance from the anal verge and tumour surface area was 5.8 (2-9)cm and 34 (0.3-152)cm2 respectively. One case had to be converted to a conventional TEM procedure because anatomical features prohibited inserting the CAD high enough into the anal canal. All lesions were excised full thickness, however in two patients with very distal lesions (case 1 & 4), the dissection was started as partial thickness (from the dentate line to the top of the puborectal sling). As per the preference of the surgeon, the defect was intraluminally closed by a running suture in six cases. No serious intra-operative complications occurred and mean (range) operating time, measured from injection of the anal block to removal of the CAD, was 84 min (30-120). Seven patients were discharged on the first postoperative day, one patient was discharged on the third postoperative day for social reasons. Postoperative morbidity was low, with only one Clavien grade 1 complication (post-TEM fever, treated with oral antibiotics and discharged on postoperative day 1). After a mean follow up of 5 months, there has been no compromised oncological outcome. The total cost of the glove TEM port was $ 70.40 if used in conjunction with reusable (glove $ 1.29, extra small alexis $ 32.22 and CAD device $ 36.89) or or $ 151.59 if disposable ports (12mm port $ 33.11, 2 x 5mm sleeves $ 48.08 and glove TEM port $ 70.40) were used.
Conclusions: The glove TEM port is a safe, cheap and readily available tool that can be used in combination with regular laparoscopic tools for transanal resection of rectal lesions. It is surgeon friendly, economically attractive and universally applicable.
Session Number: Poster – Poster Presentations
Program Number: P058
View Poster