Walaa F Abdelmoaty, MD, MBA1, Christy M Dunst, MD, FACS2, Ahmed M Sharata, MD3, Max Fisher4, Ahmed M Zihni, MD, MPH1, Filippo Filicori, MD1, Daniel Davila Bradley, MD2, Kevin M Reavis, MD, FACS2, Lee L Swanstrom, MD, FACS2, Steven R DeMeester, MD, FACS2. 1Providence Portland Medical Center, 2The Oregon Clinic, 3Maricopa Integrated Health System, 4Washington University
Introduction: Tension is the enemy of hernia repair and a leading factor in hernia recurrence. At the hiatus, crural closure is an essential component of paraesophageal hernia (PEH) repair. Often the hiatus is very enlarged, and tension on the crural closure may be associated with the known high recurrence rate after PEH repair. The aims of this study were to 1) objectively quantify crural closure tension and to 2) determine the accuracy of the surgeon’s perception of tension during PEH repair.
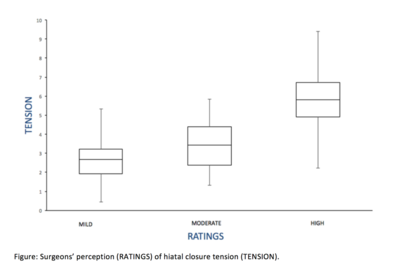
Methods and procedures: Patients undergoing laparoscopic PEH repair from June-September 2017 had the tension necessary to approximate the crura measured using a commercially available tensometer (M5-10 Force Gauge, Mark-10 Corporation, Copiague, NY, USA) and MesurGauge software (MESUR™gauge 15-1004, Mark-10 Corporation, Copiague, NY, USA) together with a Ti-Knot device (LSI Solutions, Victor, NY, USA). The measurements were digitally recorded in real time. Tension was measured at the time of Ti-Knot firing, indicated by a sharp drop of tension back to zero on the tension graph. Surgeons were asked to rate their perception of the closure tension as mild, moderate, or high for each stitch. Sutures were grouped according to location into posterior, middle, and anterior thirds of the hiatus. One-way ANOVA test was used for statistical analysis. Tension measurements are in lbf.
Results: Twenty-three patients had sixty-seven sutures placed at the hiatus. The overall median tension was 2.73 lbf. There was a steady increase in mean tension as the suture location progressed from posterior to anterior in the hiatus (posterior: 2.45 ±1.22; middle: 3.36 ± 1.36; and anterior: 3.49 ± 1.69; p=0.043). Surgeons rated the tension necessary to approximate the crura as mild in 41, moderate in 22 and high in 4 sutures. Overall, there was a significant difference in mean measured tension between the three subjective suture ratings by the surgeons. However, there was substantial variability and overlap amongst the surgeon’s ratings (Figure).
Conclusion: The tension necessary to approximate the crura during PEH repair can be objectively measured and as expected increases progressively with anterior movement up the hiatus. While there was some correlation between a surgeon’s subjective assessment of the tension necessary to bring the crura together and actual measured tension, there was wide variability and imprecision from one stitch to another. Objective tension measurement may provide a more reliable assessment of when excessive force is being used to re-approximate the crura and potentially improve PEH recurrence rates.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 87589
Program Number: P401
Presentation Session: iPoster Session (Non CME)
Presentation Type: Poster